STATISTICAL BRIEF #222 |
April 2017
Kathryn R. Fingar, Ph.D., M.P.H., Iris Mabry-Hernandez, M.D., M.P.H., Quyen Ngo-Metzger, M.D., M.P.H., Tracy Wolff, M.D., M.P.H., Claudia A. Steiner, M.D., M.P.H., and Anne Elixhauser, Ph.D. Introduction Preeclampsia is a disorder of new-onset high blood pressure occurring after 20 weeks of gestation. The diagnosis of preeclampsia is characterized by high blood pressure1 and either excess protein in the urine2 or, in the absence of proteinuria, other signs or symptoms, such as thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or cerebral or visual symptoms.3 Although rare, eclampsia occurs when women suffering from preeclampsia during pregnancy develop seizures, which may be followed by coma, posing a threat to the life of the mother and baby. 4 Women with preexisting hypertension (high blood pressure before pregnancy or within the first 20 weeks of gestation) and gestational hypertension (onset of high blood pressure after 20 weeks of gestation) are at increased risk for preeclampsia/eclampsia, although many women who develop preeclampsia/eclampsia have no history of high blood pressure. 5 Other risk factors for preeclampsia/eclampsia include preexisting diabetes, renal disease, obesity, falling in the youngest or oldest categories of maternal age, multiple gestations, women giving birth for the first time, and race.6,7 Black women are more likely to develop preeclampsia and to experience poorer outcomes associated with the condition, including progression to eclampsia and in rare cases, death.8,9 In addition to increased risk of mortality, women with preeclampsia/eclampsia are more likely to experience cesarean section (C-section), placental abruption, disseminated intravascular coagulation, cerebral hemorrhage, pulmonary edema, and renal failure.10,11,12 Infants born to mothers with preeclampsia/eclampsia are more likely to have intrauterine growth restriction, premature birth, and intrauterine death.13 In the United States, preeclampsia/eclampsia and other hypertensive disorders of pregnancy have increased over the last 2 decades.14 Preeclampsia/eclampsia is estimated to complicate between 3 and 6 percent of all pregnancies and is considered one of the most preventable causes of maternal death.15,16 However, there is little recent national population-based data on the prevalence of the condition and its associated coexisting conditions and complications that can inform efforts to prevent preeclampsia/eclampsia.17,18 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data on the prevalence of preeclampsia/eclampsia among inpatient delivery hospitalizations in 2014. The Brief describes trends in the rate of preeclampsia/eclampsia from 2005 through 2014, overall and by patient and hospital characteristics. Characteristics of deliveries with preeclampsia/eclampsia are examined in 2014. Deliveries with preeclampsia/eclampsia are compared with all other deliveries, with respect to patient and hospital characteristics, coexisting conditions, and infant and maternal outcomes.19,20 These characteristics are also compared across type of diagnosis: eclampsia, severe preeclampsia, mild or unspecified preeclampsia, and preeclampsia/eclampsia with preexisting hypertension. 21 Delivery hospitalizations represent the hospital stay for the mother and not the infant. Descriptions of infant outcomes are those conditions that appear on the maternal record. All differences between estimates noted in the text are 10 percent or greater. |
|
Findings
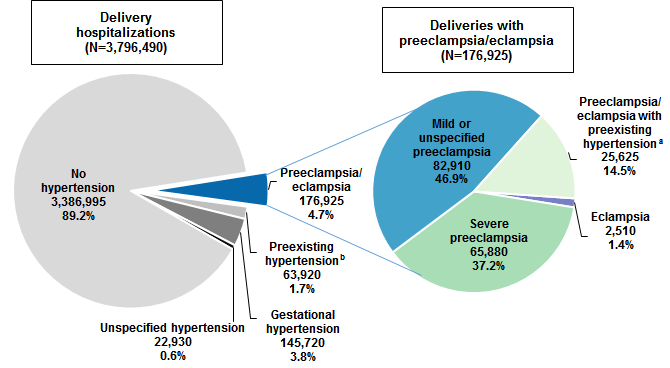
Prevalence of delivery hospitalizations involving preeclampsia/eclampsia, 2014 The left side of Figure 1 displays all delivery hospitalizations in 2014 by presence of preeclampsia/eclampsia as well as other hypertension-related diagnoses complicating pregnancy, childbirth, and the puerperium. The right side of Figure 1 displays the subset of delivery hospitalizations with a diagnosis of preeclampsia/eclampsia in 2014 by type of preeclampsia/eclampsia diagnosis. |
|
Figure 1. Hypertension-related diagnoses among delivery hospitalizations, 2014
a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. Figure 1 is two pie charts, one showing the distribution of all delivery hospitalizations with and without hypertension-related diagnoses and the other showing the distribution of deliveries by type of preeclamsia/eclampsia. Total delivery hospitalizations: 3,796,490; no hypertension: 3,386,995, 89.2%; preeclampsia, eclampsia: 176,925, 4.7%; pre-existing hypertension: 63,920, 1.7%; gestational hypertension: 145,720, 3.8%; unspecified hypertension: 22,930, 0.6%. Total deliveries with preeclampsia/eclampsia: 176,925; mild or unspecified preeclampsia: 82,910, 46.9%; severe preeclampsia: 65,880, 37.2%; preeclampsia/eclampsia with pre-existing hypertension: 25,625, 14.5%; eclampsia: 2,510, 1.4%. |
Characteristics of delivery hospitalizations involving preeclampsia/eclampsia, 2014 Table 1 compares patient and hospital characteristics among deliveries with preeclampsia/eclampsia with all other deliveries in 2014. |
| Table 1. Characteristics of deliveries with and without preeclampsia/eclampsia, 2014 | ||||||
| Patient and hospital characteristics | Preeclampsia/ eclampsia, total | All other deliveries | Type of preeclampsia/eclampsia | |||
|---|---|---|---|---|---|---|
| Eclampsia | Severe preeclampsia | Mild or unspecified preeclampsia | Preeclampsia/ eclampsia with preexisting hypertensionaa | |||
| Total, N | 176,925 | 3,619,565 | 2,510 | 65,880 | 82,910 | 25,625 |
| Patient age, mean, years | 28.5 | 28.3 | 25.8 | 28.3 | 27.8 | 31.3 |
| Patient age, years, % | ||||||
| <20 | 8.2 | 6.4 | 21.3 | 8.9 | 9.1 | 1.9 |
| 20-24 | 21.9 | 22.1 | 25.9 | 22.4 | 24.2 | 12.8 |
| 25-29 | 26.2 | 28.8 | 23.3 | 26.3 | 27.0 | 23.5 |
| 30-34 | 24.8 | 27.3 | 15.9 | 23.8 | 24.2 | 29.9 |
| 35-39 | 14.3 | 12.6 | 10.2 | 14.1 | 11.9 | 22.9 |
| 40+ | 4.6 | 2.8 | 3.4 | 4.4 | 3.5 | 8.9 |
| Race/ethnicity, % | ||||||
| White | 46.6 | 50.3 | 44.8 | 42.9 | 51.6 | 39.7 |
| Black | 20.1 | 13.1 | 23.5 | 20.8 | 16.0 | 31.3 |
| Hispanic | 19.5 | 19.4 | 19.1 | 21.1 | 19.1 | 16.7 |
| Asian/Pacific Islander | 3.4 | 5.5 | 2.2 | 3.7 | 3.2 | 3.2 |
| Other | 4.9 | 5.2 | 4.8 | 5.3 | 4.9 | 4.0 |
| Missing | 5.6 | 6.5 | 5.6 | 6.3 | 5.2 | 5.1 |
| Expected payer, % | ||||||
| Medicare | 1.0 | 0.7 | 1.2 | 1.0 | 0.7 | 1.8 |
| Medicaid | 45.2 | 42.9 | 56.8 | 45.9 | 43.1 | 49.5 |
| Private insurance | 49.2 | 50.8 | 37.0 | 48.5 | 51.5 | 44.6 |
| Uninsured | 2.1 | 2.8 | 2.6 | 2.3 | 2.1 | 1.8 |
| Other | 2.5 | 2.8 | 2.4 | 2.4 | 2.5 | 2.4 |
| Community income, % | ||||||
| Quartile 1 (poorest) | 31.9 | 27.7 | 39.6 | 32.1 | 30.3 | 36.1 |
| Quartile 2 | 26.7 | 26.5 | 24.3 | 25.8 | 27.3 | 27.3 |
| Quartile 3 | 22.9 | 24.0 | 21.9 | 23.2 | 23.4 | 20.7 |
| Quartile 4 (wealthiest) | 18.4 | 21.9 | 14.2 | 18.9 | 19.0 | 15.8 |
| Location of residence, % | ||||||
| Large metropolitan | 57.1 | 57.1 | 53.2 | 60.0 | 54.9 | 57.2 |
| Small metropolitan | 29.1 | 29.6 | 30.5 | 28.1 | 29.7 | 29.4 |
| Micropolitan | 8.2 | 8.0 | 8.8 | 6.9 | 9.3 | 7.8 |
| Rural (noncore) | 5.6 | 5.3 | 7.6 | 4.9 | 6.1 | 5.6 |
| Hospital region, % | ||||||
| Northeast | 15.5 | 16.0 | 12.7 | 16.4 | 15.0 | 14.9 |
| Midwest | 20.3 | 21.3 | 18.5 | 20.3 | 20.5 | 19.4 |
| South | 42.6 | 38.3 | 48.6 | 40.8 | 42.5 | 46.9 |
| West | 21.7 | 24.3 | 20.1 | 22.5 | 22.0 | 18.7 |
| Length of stay, mean, days | 4.4 | 2.6 | 4.4 | 4.8 | 3.7 | 5.4 |
| Cost per stay, mean, $ | 7,500 | 4,400 | 9,000 | 8,500 | 6,300 | 8,900 |
| a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||||||
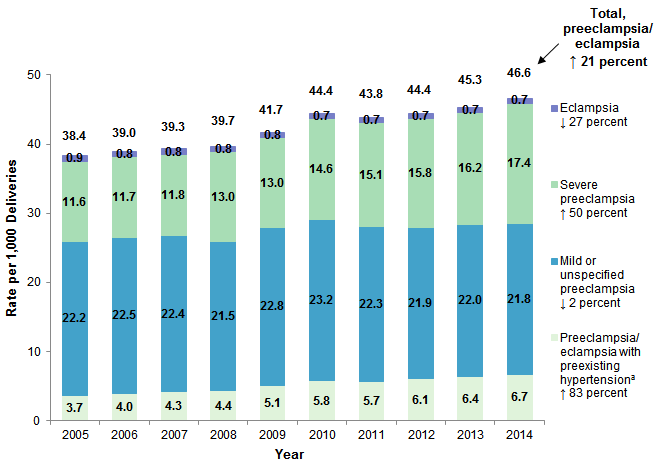
Rate of preeclampsia/eclampsia among delivery hospitalizations, 2005-2014 Figure 2 displays the rate of preeclampsia/eclampsia per 1,000 deliveries by type of diagnosis from 2005 through 2014. |
|
Figure 2. Rate of preeclampsia/eclampsia among delivery hospitalizations, 2005-2014
a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. Figure 2 is a bar chart that shows the rate of preeclampsia/eclampsia per 1,000 delivery hospitalizations by diagnosis type from 2005 through 2014. 2005: total, 38.4; preeclampsia/eclampsia with pre-existing hypertension, 3.7; mild or unspecified preeclampsia, 22.2; severe preeclampsia, 11.6; eclampsia, 0.9. 2006: total, 39.0; preeclampsia/eclampsia with pre-existing hypertension, 4.0; mild or unspecified preeclampsia, 22.5; severe preeclampsia, 11.7; eclampsia, 0.8. 2007: total, 39.3; preeclampsia/eclampsia with pre-existing hypertension, 4.3; mild or unspecified preeclampsia, 22.4; severe preeclampsia, 11.8; eclampsia, 0.8. 2008: total, 39.7; preeclampsia/eclampsia with pre-existing hypertension, 4.4; mild or unspecified preeclampsia, 21.5; severe preeclampsia, 13.0; eclampsia, 0.8. 2009: total, 41.7; preeclampsia/eclampsia with pre-existing hypertension, 5.1; mild or unspecified preeclampsia, 22.8; severe preeclampsia, 13.0; eclampsia, 0.8. 2010: total, 44.4; preeclampsia/eclampsia with pre-existing hypertension, 5.8; mild or unspecified preeclampsia, 23.2; severe preeclampsia, 14.6; eclampsia, 0.7. 2011: total, 43.8; preeclampsia/eclampsia with pre-existing hypertension, 5.7; mild or unspecified preeclampsia, 22.3; severe preeclampsia, 15.1; eclampsia, 0.7. 2012: total, 44.4; preeclampsia/eclampsia with pre-existing hypertension, 6.1; mild or unspecified preeclampsia, 21.9; severe preeclampsia, 15.8; eclampsia, 0.7. 2013: total, 45.3; preeclampsia/eclampsia with pre-existing hypertension, 6.4; mild or unspecified preeclampsia, 22.0; severe preeclampsia, 16.2; eclampsia, 0.7. 2014: total, 46.6; preeclampsia/eclampsia with pre-existing hypertension, 6.7; mild or unspecified preeclampsia, 21.8; severe preeclampsia, 17.4; eclampsia, 0.7. Percent change: total, +21%; preeclampsia/eclampsia with pre-existing hypertension, +83%; mild or unspecified preeclampsia, -2%; severe preeclampsia, +50%; eclampsia, -27%. |
Table 2 presents the total rate of preeclampsia/eclampsia per 1,000 deliveries in 2005 and 2014, by patient and hospital characteristics. |
| Table 2. Number and rate of preeclampsia/eclampsia deliveries by patient and hospital characteristics, 2005 and 2014 | |||||
| Patient and hospital characteristics | 2005 | 2014 | Percent change in rate, 2005-2014 | ||
|---|---|---|---|---|---|
| Number of deliveries with preeclampsia/ eclampsia, N | Rate of preeclampsia/ eclampsia per 1,000 deliveries | Number of deliveries with preeclampsia/ eclampsia, N | Rate of preeclampsia/ eclampsia per 1,000 deliveries | ||
| Total | 155,839 | 38.4 | 176,925 | 46.6 | 21 |
| Patient age, years | |||||
| <20 | 21,520 | 52.0 | 14,495 | 59.3 | 14 |
| 20-24 | 39,355 | 39.3 | 38,795 | 46.2 | 18 |
| 25-29 | 37,933 | 34.5 | 46,285 | 42.5 | 23 |
| 30-34 | 32,240 | 34.2 | 43,860 | 42.6 | 25 |
| 35-39 | 18,708 | 38.7 | 25,320 | 52.5 | 36 |
| 40+ | 6,068 | 54.1 | 8,170 | 73.5 | 36 |
| Expected payera | |||||
| Medicare | 1,117 | 53.4 | 1,740 | 63.9 | 20 |
| Medicaid | 69,766 | 41.2 | 79,805 | 49.0 | 19 |
| Private insurance | 75,169 | 35.8 | 86,770 | 45.1 | 26 |
| Uninsured | 5,224 | 35.9 | 3,770 | 36.2 | 1 |
| Community income | |||||
| Quartile 1 (poorest) | 46,904 | 44.3 | 55,360 | 53.2 | 20 |
| Quartile 2 | 39,444 | 40.1 | 46,325 | 46.8 | 17 |
| Quartile 3 | 36,939 | 36.7 | 39,765 | 44.5 | 21 |
| Quartile 4 (wealthiest) | 28,354 | 30.8 | 31,915 | 39.4 | 28 |
| Location of residence | |||||
| Large metropolitan | 85,752 | 37.8 | 100,810 | 46.7 | 23 |
| Small metropolitan | 43,582 | 37.2 | 51,325 | 45.8 | 23 |
| Micropolitan | 15,808 | 42.6 | 14,420 | 47.6 | 12 |
| Rural (noncore) | 10,206 | 43.7 | 9,880 | 48.7 | 12 |
| Hospital region | |||||
| Northeast | 25,572 | 34.6 | 27,350 | 45.0 | 30 |
| Midwest | 32,663 | 38.6 | 35,845 | 44.4 | 15 |
| South | 66,200 | 43.1 | 75,365 | 51.6 | 20 |
| West | 31,405 | 33.6 | 38,365 | 41.7 | 24 |
| a Other payers are not shown. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2005 and 2014 | |||||
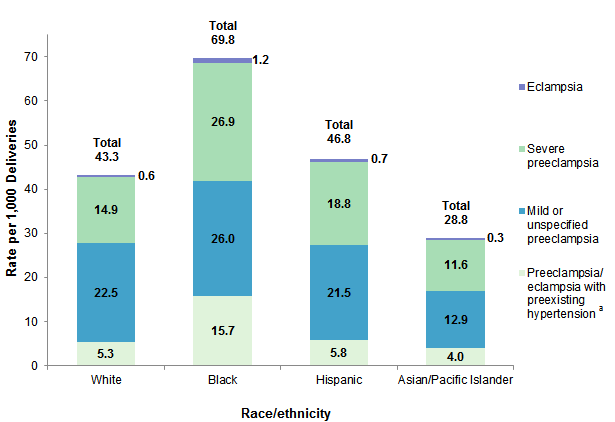
Figure 3 presents the rate of preeclampsia/eclampsia per 1,000 deliveries in 2014, by race/ethnicity and type of diagnosis. |
|
Figure 3. Rate of preeclampsia/eclampsia per 1,000 deliveries, by race/ethnicity and type of diagnosis, 2014
Notes: Trends by race/ethnicity are not shown because in 2005 a number of States did not contribute data on race/ethnicity, resulting in 26 percent of records with missing data. By 2014, the percentage of delivery records with missing data on race/ethnicity was only 6 percent. "Other" and missing races/ethnicities are not shown. Figure 3 is a bar chart that shows the rate of preeclampsia per 1,000 deliveries by race/ethnicity and diagnosis type in 2014. White: total, 43.3; preeclampsia/eclampsia with pre-existing hypertension, 5.3; mild or unspecified preeclampsia, 22.5; severe preeclampsia, 14.9; eclampsia, 0.6. Black: total, 69.8; preeclampsia/eclampsia with pre-existing hypertension, 15.7; mild or unspecified preeclampsia, 26.0; severe preeclampsia, 26.9; eclampsia, 1.2. Hispanic: total, 46.8; preeclampsia/eclampsia with pre-existing hypertension, 5.8; mild or unspecified preeclampsia, 21.5; severe preeclampsia, 18.8; eclampsia, 0.7. Asian/Pacific Islander: total, 28.8; preeclampsia/eclampsia with pre-existing hypertension, 4.0; mild or unspecified preeclampsia, 12.9; severe preeclampsia, 11.6; eclampsia, 0.3.
|
Table 3 examines each type of preeclampsia/eclampsia as a percentage of total deliveries with any preeclampsia/eclampsia by race/ethnicity. |
| Table 3. Percentage of each type of preeclampsia/eclampsia, by race/ethnicity, 2014 | ||||
| Type of preeclampsia/eclampsia | White, % | Black, % | Hispanic, % | Asian/Pacific Islander, % |
|---|---|---|---|---|
| Total | 100.0 | 100.0 | 100.0 | 100.0 |
| Eclampsia | 1.4 | 1.7 | 1.4 | 0.9 |
| Severe preeclampsia | 34.3 | 38.5 | 40.3 | 40.4 |
| Mild or unspecified preeclampsia | 51.9 | 37.3 | 45.9 | 44.9 |
| Preeclampsia/eclampsia with preexisting hypertensiona | 12.3 | 22.5 | 12.4 | 13.8 |
| a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||||
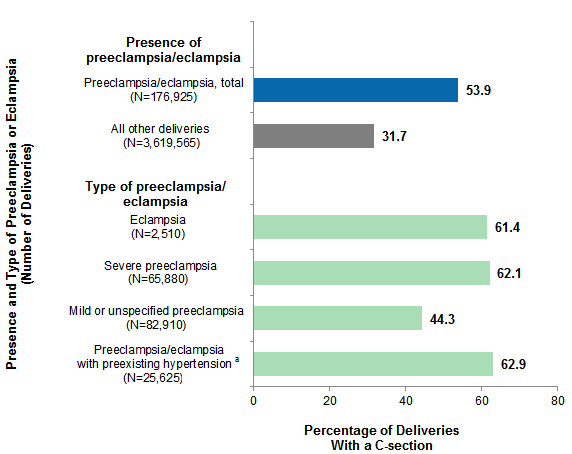
Coexisting conditions and outcomes among deliveries with preeclampsia/eclampsia, 2014 Figure 4 displays the percentage of deliveries that resulted in C-section in 2014, according to the presence and type of preeclampsia/eclampsia. |
|
Figure 4. Prevalence of C-section among deliveries with preeclampsia/eclampsia, compared with all other deliveries, 2014
Abbreviation: C-section, cesarean section Figure 4 shows the percentage of cesarean sections among deliveries with preeclampsia/eclampsia in 2014 compared with all other deliveries and by type of preeclampsia or eclampsia. Total preeclampsia/eclampsia deliveries: 53.9%; all other deliveries: 31.7%. Eclampsia: 61.4%; severe preeclampsia: 62.1%; mild or unspecified preeclampsia: 44.3%; preeclampsia/eclampsia with pre-existing hypertension: 62.9%.
|
Table 4 presents selected coexisting conditions for deliveries with preeclampsia/eclampsia, compared with all other deliveries, in 2014. The conditions displayed were chosen on the basis of prior literature and sorted according to their prevalence among deliveries with preeclampsia/eclampsia. |
| Table 4. Coexisting conditions among deliveries with preeclampsia/eclampsia, compared with all other deliveries, 2014 | ||||||
| Coexisting condition | Preeclampsia/ eclampsia, total | All other deliveries | Type of preeclampsia/eclampsia | |||
|---|---|---|---|---|---|---|
| Eclampsia | Severe preeclampsia | Mild or unspecified preeclampsia | Preeclampsia/ eclampsia with preexisting hypertensiona | |||
| Total, N | 176,925 | 3,619,565 | 2,510 | 65,880 | 82,910 | 25,625 |
| Coexisting condition, % | ||||||
| Anemia | 20.6 | 13.7 | 26.7 | 22.5 | 18.7 | 21.1 |
| Obesity | 17.3 | 6.7 | 7.8 | 15.5 | 14.1 | 33.2 |
| Gestational diabetes | 11.5 | 6.7 | 9.6 | 10.2 | 10.9 | 17.1 |
| Multiple gestations | 6.0 | 1.7 | 4.8 | 7.4 | 5.3 | 4.6 |
| Thyroid dysfunction | 4.9 | 3.6 | 3.2 | 5.4 | 4.1 | 6.4 |
| Preexisting diabetes | 4.7 | 1.0 | 2.2 | 4.4 | 3.0 | 11.4 |
| Cardiovascular disorders | 2.2 | 0.8 | 3.4 | 2.4 | 1.4 | 3.8 |
| a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||||||
Table 5 presents select outcomes for deliveries with preeclampsia/eclampsia, compared with all other deliveries, in 2014. The conditions displayed were chosen on the basis of prior literature, grouped according to whether they were identified using procedure codes or diagnosis codes pertaining to the mother or infant, and sorted according to their prevalence among deliveries with preeclampsia/eclampsia. |
| Table 5. Outcomes among deliveries with preeclampsia/eclampsia, compared with all other deliveries, 2014 | ||||||
| Delivery outcomes | Preeclampsia/ eclampsia, total | All other deliveries | Type of preeclampsia/eclampsia | |||
|---|---|---|---|---|---|---|
| Eclampsia | Severe preeclampsia | Mild or unspecified preeclampsia | Preeclampsia/ eclampsia with preexisting hypertensiona | |||
| Total, N | 176,925 | 3,619,565 | 2,510 | 65,880 | 82,910 | 25,625 |
| Delivery outcomes, number per 1,000 total deliveries | ||||||
| Procedures | ||||||
| Red blood cell or platelet transfusion | 42.7 | 10.5 | 79.7 | 63.5 | 26.9 | 36.9 |
| Ventilation | 5.3 | 0.5 | 69.7 | 6.1 | 1.6 | 8.6 |
| Hysterectomy | 1.6 | 1.0 | 6.0 | 1.7 | 0.9 | 2.9 |
| Maternal diagnoses | ||||||
| Early onset of labor | 160.5 | 54.5 | 167.3 | 234.5 | 87.3 | 206.2 |
| Placental abruption | 23.8 | 9.9 | 57.8 | 32.9 | 14.7 | 26.3 |
| Disseminated intravascular coagulation | 9.9 | 2.6 | 33.9 | 15.3 | 5.7 | 7.8 |
| Renal failure | 9.3 | 0.4 | 31.9 | 14.5 | 2.8 | 14.6 |
| Heart failure | 5.4 | 1.6 | —b | 7.2 | 3.1 | 8.2 |
| Adult respiratory distress syndrome | 4.1 | 0.4 | 39.8 | 5.5 | 1.3 | 5.9 |
| Peripartum cardiomyopathy | 2.9 | 0..4 | 6.0 | 3.0 | 1.1 | 8.4 |
| Pulmonary edema | 1.4 | 0.1 | —b | 2.2 | 0.5 | 2.1 |
| Shock | 1.2 | 0.5 | 8.0 | 2.0 | 0.3 | 1.6 |
| Puerperal cerebrovascular disorders | 1.2 | 0.3 | 12.0 | 1.4 | 0.5 | 1.8 |
| Deep venous thrombosis | 1.1 | 0.6 | —b | 1.5 | 0.7 | 1.2 |
| Sepsis | 1.0 | 0.4 | —b | 1.4 | 0.5 | 1.6 |
| Pulmonary embolism | 0.8 | 0.2 | —b | 1.2 | 0.5 | 1.0 |
| Severe anesthesia complications | 0.4 | 0.1 | —b | 0.8 | —b | —b |
| In-hospital death | 0.3 | 0.0 | —b | 0.4 | —b | —b |
| Infant-related diagnoses on the maternal record | ||||||
| Poor fetal growth | 74.6 | 25.9 | 53.8 | 101.5 | 44.9 | 103.2 |
| Intrauterine death | 11.6 | 6.2 | 27.9 | 15.5 | 6.1 | 18.0 |
| Fetal distress | 1.8 | 1.2 | —b | 1.7 | 1.8 | 1.6 |
| a Records with ICD-9-CM diagnosis code 642.7, which indicates that preeclampsia or eclampsia was present with preexisting hypertension but does not specify the severity of the condition. b Suppressed because of cell size <11 records. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||||||
Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS), 2014. Historical data were drawn from the 2005-2013 National (Nationwide) Inpatient Sample (NIS). Definitions Diagnoses, procedures, ICD-9-CM, Clinical Classifications Software (CCS), and diagnosis-related groups (DRGs) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. All-listed procedures include all procedures performed during the hospital stay, whether for definitive treatment or for diagnostic or exploratory purposes. The first-listed procedure is the procedure that is listed first on the discharge record. Inpatient data define this as the principal procedure—the procedure that is performed for definitive treatment rather than for diagnostic or exploratory purposes (i.e., the procedure that was necessary to take care of a complication). ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses and procedures. There are approximately 14,000 ICD-9-CM diagnosis codes. There are approximately 4,000 ICD-9-CM procedure codes. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.22 This clinical grouper makes it easier to quickly understand patterns of diagnoses. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. DRGs comprise a patient classification system that categorizes patients into groups that are clinically coherent and homogeneous with respect to resource use. DRGs group patients according to diagnosis, type of treatment (procedure), age, and other relevant criteria. Each hospital stay has one assigned DRG. Case definition The DRG and ICD-9-CM diagnosis codes used to identify delivery hospitalizations—overall and those with preeclampsia, eclampsia, and other types of hypertension complicating pregnancy, childbirth, and the puerperium—are shown in Tables 6 through 8. |
| Table 6. DRG codes defining delivery hospitalizations and delivery method | ||
| DRG January 2005-September 2007 | DRG October 2007-December 2013 | Description |
|---|---|---|
| 370 | 765 | C-section w/ CC/MCC |
| 371 | 766 | C-section w/o CC/MCC |
| 374 | 767 | Vaginal delivery w/ssterilization and/or D&C |
| 375 | 768 | Vaginal delivery w/ other OR procedure |
| 372 | 774 | Vaginal delivery w/ CC/MCC |
| 373 | 775 | Vaginal delivery w/o CC/MCC |
| Abbreviations: CC, complications or comorbidities; MCC, major complications or comorbidities; D&C, dilation and curettage; OR, operating room | ||
| Table 7. ICD-9-CM diagnosis codes defining preeclampsia/eclampsia and other types of hypertension complicating pregnancy, childbirth, and the puerperium | ||
| ICD-9-CM diagnosis code | Description | Type of hypertensiona |
|---|---|---|
| 642.0x | Benign essential hypertension complicating pregnancy, childbirth, and the puerperium | Preexisting |
| 642.1x | Hypertension secondary to renal disease, complicating pregnancy, childbirth, and the puerperium | |
| 642.2x | Other pre-existing hypertension complicating pregnancy, childbirth, and the puerperium | |
| 642.3x | Transient hypertension of pregnancy | Gestational |
| 642.9x | Unspecified hypertension complicating pregnancy, childbirth, and the puerperium | Unspecified |
| 642.4x | Mild or unspecified pre-eclampsia | Preeclampsia/ eclampsia |
| 642.5x | Severe pre-eclampsia | |
| 642.6x | Eclampsia | |
| 642.7x | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension | |
| a Records with multiple codes were assigned to one category using the following hierarchy: preeclampsia/eclampsia, preexisting hypertension, gestational, unspecified. | ||
| Table 8. ICD-9-CM diagnosis codes defining types of preeclampsia/eclampsia | ||
| ICD-9-CM diagnosis code | Description | Type of hypertensiona |
|---|---|---|
| 642.40 | Mild or unspecified pre-eclampsia, unspecified as to episode of care or not applicable | Mild or unspecified preeclampsia |
| 642.41 | Mild or unspecified pre-eclampsia, delivered, with or without mention of antepartum condition | |
| 642.42 | Mild or unspecified pre-eclampsia, delivered, with mention of postpartum complication | |
| 642.43 | Mild or unspecified pre-eclampsia, antepartum condition or complication | |
| 642.44 | Mild or unspecified pre-eclampsia, postpartum condition or complication | |
| 642.50 | Severe pre-eclampsia, unspecified as to episode of care or not applicable | Severe preeclampsia |
| 642.51 | Severe pre-eclampsia, delivered, with or without mention of antepartum condition | |
| 642.52 | Severe pre-eclampsia, delivered, with mention of postpartum complication | |
| 642.53 | Severe pre-eclampsia, antepartum condition or complication | |
| 642.54 | Severe pre-eclampsia, postpartum condition or complication | |
| 642.60 | Eclampsia, unspecified as to episode of care or not applicable | Eclampsia |
| 642.61 | Eclampsia, delivered, with or without mention of antepartum condition | |
| 642.62 | Eclampsia, delivered, with mention of postpartum complication | |
| 642.63 | Eclampsia, antepartum condition or complication | |
| 642.64 | Eclampsia, postpartum condition or complication | |
| 642.70 | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension, unspecified as to episode of care or not applicable | Preeclampsia/ eclampsia with preexisting hypertension |
| 642.71 | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension, delivered, with or without mention of antepartum condition | |
| 642.72 | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension, delivered, with mention of postpartum complication | |
| 642.73 | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension, antepartum condition or complication | |
| 642.74 | Pre-eclampsia or eclampsia superimposed on pre-existing hypertension, postpartum condition or complication | |
| a Records with multiple codes were assigned to one category using the following hierarchy: eclampsia, severe preeclampsia, mild or unspecified preeclampsia, preeclampsia or eclampsia with preexisting hypertension. | ||
ICD-9-CM diagnosis codes identifying coexisting conditions and maternal and infant outcomes are provided in Tables 9 and 10. Codes came from both Chapter 11 of the ICD manual on Complications of Pregnancy, Childbirth, and the Puerperium (ICD-9-CM codes 630-679), as well as from non-pregnancy-related chapters. Maternal outcomes are generally consistent with the definitions used by a prior study on severe obstetric morbidity.23
|
| Table 9. ICD-9-CM diagnosis and CCS codes defining coexisting conditions at delivery | ||
| ICD-9-CM diagnosis code or CCS category | Description | Condition |
|---|---|---|
| 648.2 | Anemia | Anemia |
| 280 | Iron deficiency anemias | |
| 281 | Other deficiency anemias | |
| 282 | Hereditary hemolytic anemias | |
| 283 | Acquired hemolytic anemias | |
| 284 | Aplastic anemia and other bone marrow failure syndromes | |
| 285 | Other and unspecified anemias | |
| 648.5 | Congenital cardiovascular disorders | Cardiovascular disorders |
| 648.6 | Other cardiovascular diseases | |
| 745 | Bulbus cordis anomalies and anomalies of cardiac septal closure | |
| 746 | Other congenital anomalies of heart | |
| 747 | Other congenital anomalies of circulatory system | |
| 390-392 | Acute rheumatic fever | |
| 393-398 | Chronic rheumatic heart disease | |
| 410-414 | Ischemic heart disease | |
| 415-417 | Diseases of pulmonary circulation | |
| 420-429 | Other forms of heart disease | |
| 648.8 | Abnormal glucose tolerance | Gestational diabetesa |
| 651 | Multiple gestation | Multiple gestations |
| V27.2 | Twins, both liveborn | |
| V27.3 | Twins, one liveborn and one stillborn | |
| V27.4 | Twins, both stillborn | |
| V27.5 | Other multiple birth, all liveborn | |
| V27.6 | Other multiple birth, some liveborn | |
| V27.7 | Other multiple birth, all stillborn | |
| 649.1 | Obesity complicating pregnancy, childbirth, or the puerperium | Obesity |
| 278.0 | Overweight and obesity | |
| V85.2 | Body Mass Index between 25-29, adult | |
| V85.3 | Body Mass Index between 30-39, adult | |
| V85.4 | Body Mass Index 40 and over, adult | |
| 648.0 | Diabetes mellitus | Preexisting diabetes |
| CCS 49 | Diabetes mellitus without complications | |
| CCS 50 | Diabetes mellitus with complications | |
| 648.1 | Thyroid dysfunction | Thyroid dysfunction |
| 240-246 | Disorders of thyroid gland | |
| Abbreviation: CCS: Clinical Classifications Software a Records with codes for both preexisting and gestational diabetes were categorized as preexisting diabetes. | ||
| Table 10. ICD-9-CM procedure codes defining maternal and infant outcomes at delivery | ||
| ICD-9-CM procedure code | Description | Outcome |
|---|---|---|
| Procedures | ||
| 68.3 | Subtotal abdominal hysterectomy | Hysterectomya |
| 68.4 | Total abdominal hysterectomy | |
| 68.5 | Vaginal hysterectomy | |
| 68.6 | Radical abdominal hysterectomy | |
| 68.7 | Radical vaginal hysterectomy | |
| 68.8 | Pelvic evisceration | |
| 68.9 | Other and unspecified hysterectomy | |
| 99.04 | Transfusion of packed cells | Red blood cell or platelet transfusion |
| 99.05 | Transfusion of platelets | |
| 93.90 | Non-invasive mechanical ventilation | Ventilationa |
| 96.01 | Insertion of nasopharyngeal airway | |
| 96.02 | Insertion of oropharyngeal airway | |
| 96.03 | Insertion of esophageal obturator airway | |
| 96.04 | Insertion of endotracheal tube | |
| 96.05 | Other intubation of respiratory tract | |
| 96.7 | Other continuous invasive mechanical ventilation | |
| Maternal diagnoses | ||
| 518.5 | Pulmonary insufficiency following trauma and surgery | Adult respiratory distress syndromea |
| 518.81 | Acute respiratory failure | |
| 518.82 | Other pulmonary insufficiency, not elsewhere classified | |
| 518.84 | Acute and chronic respiratory failure | |
| 671.3 | Deep phlebothrombosis, antepartum | Deep venous thrombosisa |
| 671.4 | Deep phlebothrombosis, postpartum | |
| 671.9 | Unspecified venous complication | |
| 451 | Phlebitis and thrombophlebitis | |
| 452 | Portal vein thrombosis | |
| 453 | Other venous embolism and thrombosis | |
| 666.3 | Postpartum coagulation defects | Disseminated intravascular coagulationa |
| 286.6 | Defibrination syndrome | |
| 286.9 | Other and unspecified coagulation defects | |
| 644.2 | Early onset of delivery | Early onset of labor |
| 669.4 | Other complications of obstetrical surgery and procedures | Heart failurea |
| 427.5 | Cardiac arrest | |
| 428.1 | Left heart failure | |
| 428.21 | Systolic heart failure, acute | |
| 428.31 | Diastolic heart failure, acute | |
| 428.41 | Combined systolic and diastolic heart failure, acute | |
| 997.1 | Cardiac complications | |
| 674.5 | Peripartum cardiomyopathy | Peripartum cardiomyopathy |
| 425 | Cardiomyopathy | |
| 641.2 | Abruptio placenta | Placental abruption |
| 674.0 | Cerebrovascular disorders in the puerperium | Puerperal cerebrovascular disordersa |
| 671.5 | Other phlebitis and thrombosis | |
| 430 | Subarachnoid hemorrhage | |
| 431 | Intracerebral hemorrhage | |
| 432 | Other and unspecified intracranial hemorrhage | |
| 433 | Occlusion and stenosis of precerebral arteries | |
| 434 | Occlusion of cerebral arteries | |
| 436 | Acute, but ill-defined, cerebrovascular disease | |
| 437 | Other and ill-defined cerebrovascular disease | |
| 997.2 | Peripheral vascular complications | |
| 999.2 | Other vascular complications | |
| 518.4 | Acute edema of lung, unspecified | Pulmonary edemaa |
| 428.1 | Left heart failure | |
| 673 | Obstetrical pulmonary embolism | Pulmonary embolisma |
| 415.1 | Pulmonary embolism and infarction | |
| 669.3 | Acute renal failure following labor and delivery | Renal failurea |
| 584 | Acute renal failure | |
| 038 | Septicemia | Sepsisa |
| 995.1 | Sepsis | |
| 995.2 | Severe sepsis | |
| 668.0 | Pulmonary complications following administration of anesthetic or other sedation in labor and delivery | Severe anesthesia complicationsa |
| 668.1 | Cardiac complications following administration of anesthetic or other sedation in labor and delivery | |
| 668.2 | Central nervous system complications following administration of anesthetic or other sedation in labor and delivery | |
| 669.1 | Shock during or following labor and delivery | Shocka |
| 998.0 | Postoperative shock | |
| 995.0 | Other anaphylactic shock | |
| 995.4 | Shock due to anesthesia | |
| 785.5 | Shock without mention of trauma | |
| Infant-related diagnoses on the maternal record | ||
| 656.3 | Fetal distress | Fetal distress |
| 656.4 | Intrauterine death | Intrauterine death |
| V27.1 | Single, stillborn | |
| V27.3 | Twins, one liveborn and one stillborn | |
| V27.4 | Twins, both stillborn | |
| V27.6 | Other multiple birth, some liveborn | |
| V27.7 | Other multiple birth, all stillborn | |
| 656.5 | Poor fetal growth | Poor fetal growth |
| a Definition consistent with measures of severe obstetric morbidity used by Kuklina EV, Meikle SF, Jamieson DJ, Whiteman MK, Barfield WD, Hills SD, et al. Severe Obstetric Morbidity in the United States: 1998-2005. Obstetrics and Gynecology. 2009;113(2 Pt 1): 293-9. | ||
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Costs and charges Total hospital charges were converted to costs using HCUP Cost-to-Charge Ratios based on hospital accounting reports from the Centers for Medicare & Medicaid Services (CMS).24 Costs reflect the actual expenses incurred in the production of hospital services, such as wages, supplies, and utility costs; charges represent the amount a hospital billed for the case. For each hospital, a hospital-wide cost-to-charge ratio is used. Hospital charges reflect the amount the hospital billed for the entire hospital stay and do not include professional (physician) fees. For the purposes of this Statistical Brief, costs are reported to the nearest hundred. Location of patients' residence Place of residence is based on the Urban Influence Codes (UIC) for the urban-rural classification scheme for U.S. counties:
Median community-level income is the median household income of the patient's ZIP Code of residence. Income levels are separated into population-based quartiles with cut-offs determined using ZIP Code demographic data obtained from the Nielsen Company. The income quartile is missing for patients who are homeless or foreign. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
Hospital stays billed to the State Children's Health Insurance Program (SCHIP) may be classified as Medicaid, Private Insurance, or Other, depending on the structure of the State program. Because most State data do not identify patients in SCHIP specifically, it is not possible to present this information separately. For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Region Region is one of the four regions defined by the U.S. Census Bureau:
Reporting of race and ethnicity Data on Hispanic ethnicity are collected differently among the States and also can differ from the Census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other (including mixed race)) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, Asian/Pacific Islander, and non-Hispanic Other, including American Indian/Alaska Native. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About Statistical Briefs HCUP Statistical Briefs are descriptive summary reports presenting statistics on hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, patient populations, and other topics. The reports use HCUP administrative healthcare data. About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
The new sampling strategy is expected to result in more precise estimates than those that resulted from the previous NIS design by reducing sampling error: for many estimates, confidence intervals under the new design are about half the length of confidence intervals under the previous design. The change in sample design for 2012 necessitates recomputation of prior years' NIS data to enable analyses of trends that use the same definitions of discharges and hospitals. For More Information For other information on pregnancy and childbirth, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_pregnancy.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National (Nationwide) Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated December 2016. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed January 31, 2017. Suggested Citation Fingar KR (IBM Watson Health), Mabry-Hernandez I (AHRQ), Ngo-Metzger Q (AHRQ), Wolff T (AHRQ), Steiner CA (Institute for Health Research, Kaiser Permanente), Elixhauser A (AHRQ). Delivery Hospitalizations Involving Preeclampsia and Eclampsia, 2005-2014. HCUP Statistical Brief #222. April 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb222-Preeclampsia-Eclampsia-Delivery-Trends.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Sharon Arnold, Ph.D., Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on April 25, 2017. 1 >140/90 mm Hg on two occasions 4 hours apart. 2 >300 mg/dL on a 24-hour urine protein test, protein:creatinine ratio of >0.3 mg/mmol, or urine protein dipstick reading >1 if quantitative analysis is not available. 3 American College of Obstetricians and Gynecologists. Hypertension in Pregnancy. Washington, DC: American College of Obstetricians and Gynecologists; 2013. 4 Ibid. 5 Mammaro A, Carrara S, Cavaliere A, Ermito S, Dinatale A, Pappalardo EM, et al. Hypertensive disorders of pregnancy. Journal of Prenatal Medicine. 2009;3(1):1-5. 6Ibid. 7 Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. American Journal of Obstetrics & Gynecology. 2000;183:S1-S22. 8 Shahul S, Tung A, Minhaj M, Nizamuddin J, Wenger J, Mahmood E, et al. Racial disparities in comorbidities, complications, and maternal and fetal outcomes in women with preeclampsia/eclampsia. Hypertension in Pregnancy. 2015;34(4):506-15. 9Tanaka M, Jaamaa G, Kaiser M, Hills E, Soim A, Zhu M, et al. Racial disparity in hypertensive disorders of pregnancy in New York State: a 10-year longitudinal population-based study. American Journal of Public Health. 2007;97(1):163-70. 10 Ibid. 11 Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. American Journal of Obstetrics and Gynecology. 2000;183:S1-S22. 12 Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity in the United States. Obstetrics and Gynecology. 2009;113(6):1299-306. 13 Mammaro A, Carrara S, Cavaliere A, Ermito S, Dinatale A, Pappalardo EM, et al. Hypertensive disorders of pregnancy. Journal of Prenatal Medicine. 2009;3(1):1-5. 14 Centers for Disease Control and Prevention. Data on Selected Pregnancy Complications in the United States. October 2016. www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-complications-data.htm. Accessed March 29, 2017. 15 Shahul et al., 2015. Op. cit. 16 D'Alton ME, Main EK, Menard MK, Levy BS. The National Partnership for Maternal Safety. Obstetrics and Gynecology. 2014;123:973-7. 17 Ananth CV, Keyes KM, Wapner RJ. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ. 2013;347:f6564. 18 Wallis AB, Saftlas AF, Hsia J, Atrash HK. Secular trends in the rates of preeclampsia, eclampsia, and gestational hypertension, United States, 1987-2004. American Journal of Hypertension. 2008;21:521-6. 19 Kuklina EV, Meikle SF, Jamieson DJ, Whiteman MK, Barfield WD, Hills SD, et al. Severe obstetric morbidity in the United States: 1998-2005. Obstetrics and Gynecology. 2009;113(2 Pt 1):293-9. 20 Callaghan WM, Creanga AA, Kuklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstetrics and Gynecology. 2012;120(5):1029-36. 21 The first three categories are defined by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes for mild or unspecified preeclampsia (642.4), severe preeclampsia (642.5), and eclampsia (642.6). These codes are used if preexisting hypertension was not present. The last category is defined by the code 642.7, which is used if preexisting hypertension was present with preeclampsia/eclampsia. However, records with this code lack detail on the severity of preeclampsia/eclampsia. 22 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated October 2016. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed January 31, 2017. 23 Kuklina EV, Meikle SF, Jamieson DJ, Whiteman MK, Barfield WD, Hills SD, et al. Severe obstetric morbidity in the United States: 1998-2005. Obstetrics and Gynecology. 2009;113(2 Pt 1):293-9. 24 Agency for Healthcare Research and Quality. HCUP Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). 2001-2014. Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2016. www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed January 31, 2017. |
| Internet Citation: Statistical Brief #222. Healthcare Cost and Utilization Project (HCUP). April 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb222-Preeclampsia-Eclampsia-Delivery-Trends.jsp. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 4/24/17 |