STATISTICAL BRIEF #154 |
April 2013
Audrey J. Weiss, Ph.D., Anne Elixhauser, Ph.D., and Claudia Steiner, M.D., M.P.H. Introduction Readmissions—revisits to the hospital within a certain time frame following an initial inpatient stay—are receiving increasing attention as a measure of quality of care and a potential source for reducing healthcare costs.1 Although not all rehospitalizations can be prevented, many readmissions could be avoided with improvements in the quality of hospital care provided during, transitioning from, and following the inpatient stay. Research indicates that nearly one in five Medicare patients are readmitted to the hospital within 30 days, about 90 percent of these readmissions are unplanned, and the costs to Medicare are more than $17 billion.2 The Patient Protection and Affordable Care Act (Section 3025) mandates a hospital readmissions reduction program whereby Medicare payments will be reduced for hospitals with excessive readmissions.3 Prior research has offered select views of readmissions for general surgery4 or high-risk surgery,5 and some studies have focused on readmissions for specific surgical procedures such as percutaneous coronary intervention (PCI/PTCA).6,7 However, relatively limited information is available about readmissions by procedure. This Statistical Brief provides an overview of 30-day all-payer, all-cause readmissions to U.S. hospitals for a range of inpatient procedures in 2010. It presents the most comprehensive national estimates on readmissions by procedure that is available to date. In this Statistical Brief, readmission was defined as a subsequent hospital admission within 30 days following an original admission (or index stay) with a major operating room procedure that occurred from January through November 2010. All-cause readmissions were examined; thus, readmissions may or may not include procedures that were listed during the index stay. Readmissions were tracked across the same or different hospitals. Some readmissions may be planned or unavoidable-no attempt was made to remove these types of readmissions from the analysis. Readmission rates using Healthcare Cost and Utilization Project (HCUP) data are provided for the most frequent procedures treated in U.S. hospitals during 2010 and for the procedures with the highest readmission rates. All estimates were taken from HCUPnet, the online query system that provides free access to information from HCUP.8 For a subset of procedures, readmission rates are presented by age group and expected payer (insurance status). Patients younger than 1 year were excluded from this analysis. Readmission rates were calculated without risk adjustment. |
|
Appendix A provides detailed information on readmission rates for most procedures performed in U.S. hospitals in 2010. The table provides information on the number of index stays for each procedure, the number of all-cause readmissions within 30 days, and the percentage of index stays that were followed by a readmission within 30 days for any cause. Excluded were nonspecific procedures and any procedures with fewer than 5,000 index stays or fewer than 500 readmissions. In general, procedures are organized by body system in this table.
Findings Readmission rates for the most frequent procedures Table 1 lists the 30 most frequent procedures performed in U.S. hospitals, with their 30-day readmission rates. Readmission rates for these high-volume procedures varied from a low of 2.0 percent (Cesarean section and ligation of fallopian tubes) to a high of 22.8 percent (amputation of a lower extremity). The most frequent procedures and their readmission rates were Cesarean section (2.0 percent), knee arthroplasty (5.0 percent), percutaneous coronary angioplasty (12.9 percent), laminectomy (6.7 percent), and spinal fusion (6.8 percent). Among the most frequent procedures, as many as one in five patients were readmitted within 30 days. The highest readmission rates were for amputation of a lower extremity (22.8 percent); debridement of a wound, infection, or burn (19.1 percent); heart valve procedures (18.5 percent); and small bowel resection (18.1 percent). The lowest readmission rates were for procedures related to childbirth and the reproductive organs (Cesarean section, 2.0 percent; ligation of fallopian tubes, 2.0 percent; repair of cystole and rectocele, obliteration of vaginal vault, 2.6 percent) or genitourinary incontinence (3.0 percent). Procedures with the highest readmission rates Table 2 lists procedures ranked by the highest readmission rates. Diagnostic procedures (e.g., exploratory surgery, biopsy) and nonspecific categories are excluded from this table. Diagnostic procedures are included in the Appendix. Across all inpatient procedures, 30-day readmission rates reached a high of almost one in three patients for kidney transplant (29.1 percent) and ileostomy and other enterostomy (29.1 percent). Three other procedures—those to create access for hemodialysis (27.4 percent), nephrotomy and nephrostomy (24.0 percent), and tracheostomy (23.9 percent)—had readmission rates of approximately one in four patients. |
| Table 1. All-cause 30-day readmissions ranked by the most frequent procedures* performed during the index stay, U.S. hospitals, 2010 | ||||
| Rank | All-listed procedure for index hospital stay** | Number of index stays | 30-day all-cause readmissions | |
|---|---|---|---|---|
| Number of readmissions | Percent readmitted | |||
| 1 | Cesarean section | 1,209,422 | 24,281 | 2.0 |
| 2 | Arthroplasty knee | 651,965 | 32,764 | 5.0 |
| 3 | Percutaneous coronary angioplasty (PTCA) | 603,446 | 78,038 | 12.9 |
| 4 | Laminectomy, excision intervertebral disc | 456,664 | 30,383 | 6.7 |
| 5 | Spinal fusion | 431,577 | 29,326 | 6.8 |
| 6 | Hip replacement, total and partial | 424,408 | 34,265 | 8.1 |
| 7 | Cholecystectomy and common duct | 419,433 | 39,774 | 9.5 |
| 8 | Hysterectomy, abdominal and vaginal | 409,674 | 19,446 | 4.7 |
| 9 | Excision, lysis peritoneal adhesions | 342,425 | 42,126 | 12.3 |
| 10 | Appendectomy | 315,034 | 18,835 | 6.0 |
| 11 | Partial excision bone | 307,221 | 30,810 | 10.0 |
| 12 | Colorectal resection | 294,071 | 43,388 | 14.8 |
| 13 | Oophorectomy, unilateral and bilateral | 288,228 | 17,480 | 6.1 |
| 14 | Treatment, fracture or dislocation of hip and femur | 278,118 | 33,049 | 11.9 |
| 15 | Ligation of fallopian tubes | 238,190 | 4,819 | 2.0 |
| 16 | Coronary artery bypass graft (CABG) | 234,840 | 35,484 | 15.1 |
| 17 | Treatment, fracture or dislocation of lower extremity (other than hip or femur) | 194,033 | 15,816 | 8.2 |
| 18 | Insertion, revision, replacement, removal of cardiac pacemaker or cardioverter/defibrillator | 149,147 | 23,057 | 15.5 |
| 19 | Debridement of wound, infection or burn | 148,544 | 28,394 | 19.1 |
| 20 | Intraoperative cholangiogram | 134,934 | 11,551 | 8.6 |
| 21 | Amputation of lower extremity | 124,880 | 28,488 | 22.8 |
| 22 | Heart valve procedures | 110,615 | 20,502 | 18.5 |
| 23 | Incision and excision of the central nervous system (CNS) | 105,700 | 17,019 | 16.1 |
| 24 | Skin graft | 97,756 | 14,789 | 15.1 |
| 25 | Endarterectomy, vessel of head and neck | 96,711 | 9,233 | 9.5 |
| 26 | Repair of cystocele and rectocele, obliteration of vaginal vault | 95,703 | 2,487 | 2.6 |
| 27 | Transurethral excision, drainage, or removal urinary obstruction | 88,139 | 11,795 | 13.4 |
| 28 | Small bowel resection | 83,157 | 15,050 | 18.1 |
| 29 | Lobectomy or pneumonectomy | 82,264 | 9,431 | 11.5 |
| 30 | Genitourinary incontinence procedures | 78,767 | 2,327 | 3.0 |
| Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID), 2010, Agency for Healthcare Research and Quality (AHRQ). * Information is provided for procedures with at least 5,000 weighted occurrences and 500 or more weighted readmissions. See text and Definitions for details on methods for calculating readmissions. ** Clinical Classification Software (CCS) label. Excludes diagnostic and nonspecific CCS categories. See Appendix for additional descriptions of the CCS categories. |
||||
| Table 2. All-cause 30-day readmissions ranked by the highest readmission rates for procedures* performed during the index stay, U.S. hospitals, 2010 | ||||
| Rank | All-listed procedure for index hospital stay** | Number of index stays | 30-day all-cause readmissions | |
|---|---|---|---|---|
| Number of readmissions | Percent readmitted | |||
| 1 | Kidney transplant | 16,761 | 4,882 | 29.1 |
| 2 | Ileostomy and other enterostomy (except colostomy) | 23,392 | 6,811 | 29.1 |
| 3 | Procedures to create access for hemodialysis | 49,982 | 13,682 | 27.4 |
| 4 | Nephrotomy and nephrostomy | 43,773 | 10,508 | 24.0 |
| 5 | Tracheostomy, temporary and permanent | 9,335 | 2,234 | 23.9 |
| 6 | Amputation of lower extremity | 124,880 | 28,488 | 22.8 |
| 7 | Bone marrow transplant | 12,919 | 2,905 | 22.5 |
| 8 | Embolectomy and endarterectomy of lower limbs | 44,584 | 9,387 | 21.1 |
| 9 | Peripheral vascular bypass | 72,529 | 15,005 | 20.7 |
| 10 | Insertion, replacement, or removal of extracranial ventricular shunt | 32,957 | 6,633 | 20.1 |
| 11 | Debridement of wound, infection or burn | 148,544 | 28,394 | 19.1 |
| 12 | Incision of pleura, thoracentesis, chest drainage | 13,933 | 2,648 | 19.0 |
| 13 | Colostomy, temporary and permanent | 46,675 | 8,859 | 19.0 |
| 14 | Heart valve procedures | 110,615 | 20,502 | 18.5 |
| 15 | Small bowel resection | 83,157 | 15,050 | 18.1 |
| 16 | Procedures on spleen | 23,600 | 4,162 | 17.6 |
| 17 | Incision and excision of the central nervous system (CNS) | 105,700 | 17,019 | 16.1 |
| 18 | Insertion, revision, replacement, removal of cardiac pacemaker or cardioverter/defibrillator | 149,147 | 23,057 | 15.5 |
| 19 | Skin graft | 97,756 | 14,789 | 15.1 |
| 20 | Coronary artery bypass graft (CABG) | 234,840 | 35,484 | 15.1 |
| 21 | Colorectal resection | 294,071 | 43,388 | 14.8 |
| 22 | Gastrectomy, partial and total | 34,551 | 4,728 | 13.7 |
| 23 | Excision of skin lesion | 7,404 | 1,007 | 13.6 |
| 24 | Transurethral excision, drainage, or removal urinary obstruction | 88,139 | 11,795 | 13.4 |
| 25 | Aortic resection, replacement or anastomosis | 46,861 | 6,116 | 13.1 |
| 26 | Percutaneous coronary angioplasty (PTCA) | 603,446 | 78,038 | 12.9 |
| 27 | Excision, lysis peritoneal adhesions | 342,425 | 42,126 | 12.3 |
| 28 | Treatment, fracture or dislocation of hip and femur | 278,118 | 33,049 | 11.9 |
| 29 | Lobectomy or pneumonectomy | 82,264 | 9,431 | 11.5 |
| 30 | Hemorrhoid procedures | 9,298 | 1,020 | 11.0 |
| Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID), 2010, Agency for Healthcare Research and Quality (AHRQ). * Information is provided for procedures with at least 5,000 weighted occurrences and 500 or more weighted readmissions. See text and Definitions for details on methods for calculating readmissions. ** Clinical Classification Software (CCS) label. Excludes diagnostic and nonspecific CCS categories. See Appendix for additional descriptions of the CCS categories. |
||||
Among the 30 procedures with the highest readmission rates, 14 of them also are among the 30 most frequent procedures performed in the U.S. Percutaneous coronary angioplasty (78,038 patients; 12.9 percent readmission rate) has the 26th highest readmission rate and is the 3rd most common procedure. Colorectal resection (43,388 patients; 14.8 percent readmission rate) has the 21st highest readmission rate and is the 12th most common procedure. Excision or lysis of peritoneal adhesions (42,126 patients; 12.3 percent readmission rate) has the 27th highest readmission rate and is the 9th most common procedure. CABG (35,484 patients; 15.1 percent readmission rate) has the 20th highest readmission rate and is the 16th most common procedure. Treatment of hip/femur fracture (33,049 patients; 11.9 percent readmission rate) has the 28th highest readmission rate and is the 17th most common procedure.
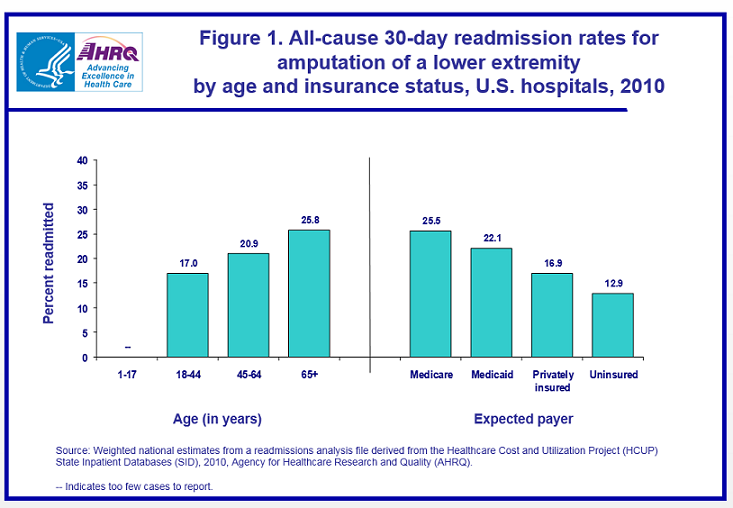
Readmission rates by age and insurance status for selected procedures Figures 1–6 provide details on 30-day all-cause readmission rates for the six procedures from Table 2 that involved more than 100,000 index stays and had overall readmission rates of at least 15 percent. Figure 1 depicts readmission rates for amputation of a lower extremity. Readmission rates increased with age, ranging from 17.0 percent among patients aged 18–44 years to 25.8 percent among patients aged 65 years and older. The highest readmission rate was seen for patients with an expected payer of Medicare (25.5 percent) compared to 22.1 percent for Medicaid-covered patients, 16.9 percent for privately insured patients, and 12.9 percent for the uninsured. |
|
Figure 1. All-cause 30-day readmission rates for amputation of a lower extremity by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, too few cases to report. Ages 18 through 44, 17 percent. Ages 45 through 64, 20.9 percent. Ages 65 and older, 25.8 percent. Medicare payer, 25.5 percent. Medicaid payer, 22.1 percent. Privately insured, 16.9 percent. Uninsured, 12.9 percent. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
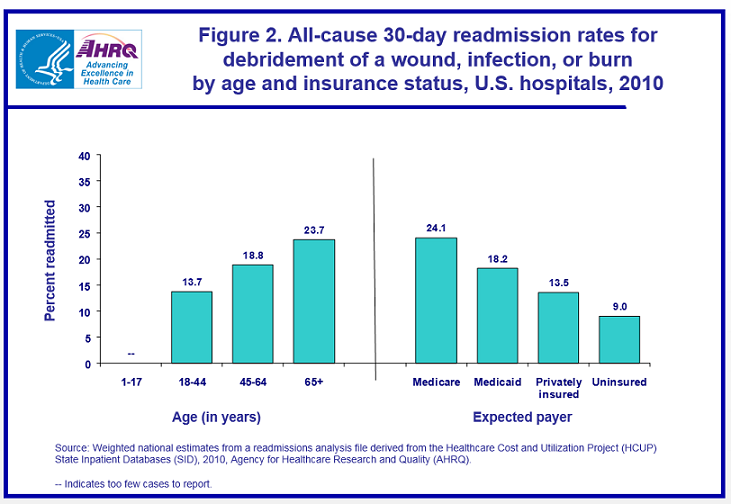
Readmission rates for debridement of a wound, infection, or burn are shown in figure 2. Readmission rates progressively were higher with advancing age, increasing from 13.7 percent for 18–44 year olds to 23.7 percent for those aged 65 years and older. The readmission rate was highest for Medicare-covered patients (24.1 percent). The readmission rate for Medicaid-covered patients was 18.2 percent and for privately insured patients it was 13.5 percent, whereas for uninsured patients it was only 9.0 percent. |
|
Figure 2. All-cause 30-day readmission rates for debridement of a wound, infection, or burn by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, too few cases to report. Ages 18 through 44, 13.7 percent. Ages 45 through 64, 18.8 percent. Ages 65 and older, 23.7 percent. Medicare payer, 24.1 percent. Medicaid payer, 18.2 percent. Privately insured, 13.5 percent. Uninsured, 9.0 percent. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
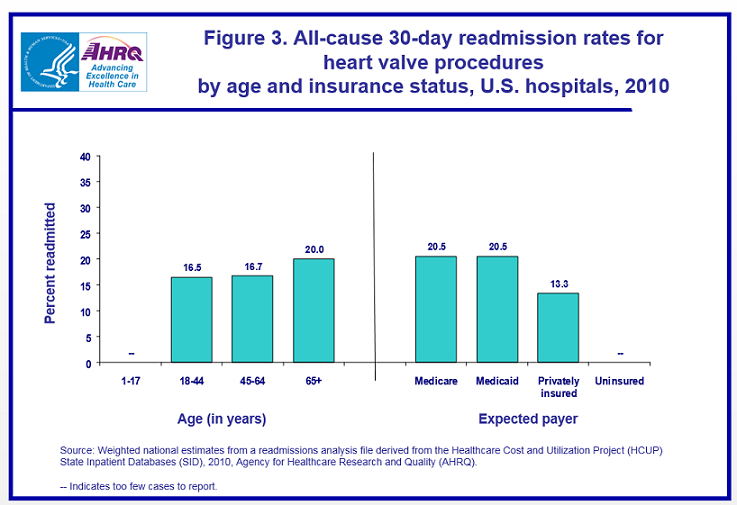
Figure 3 shows readmission rates for heart valve procedures. Readmission rates were highest for those aged 65 years and older (20.0 percent) and lower for those in the two younger age groups (16.5–16.7 percent). Readmission rates were identical for patients with an expected payer of Medicare or Medicaid (20.5 percent), which was more than 50 percent higher than for privately insured patients (13.3 percent). |
|
Figure 3. All-cause 30-day readmission rates for heart valve procedures by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, too few cases to report. Ages 18 through 44, 16.5 percent. Ages 45 through 64, 16.7 percent. Ages 65 and older, 20.0 percent. Medicare payer, 20.5 percent. Medicaid payer, 20.5 percent. Privately insured, 13.3 percent. Uninsured, too few cases to report. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
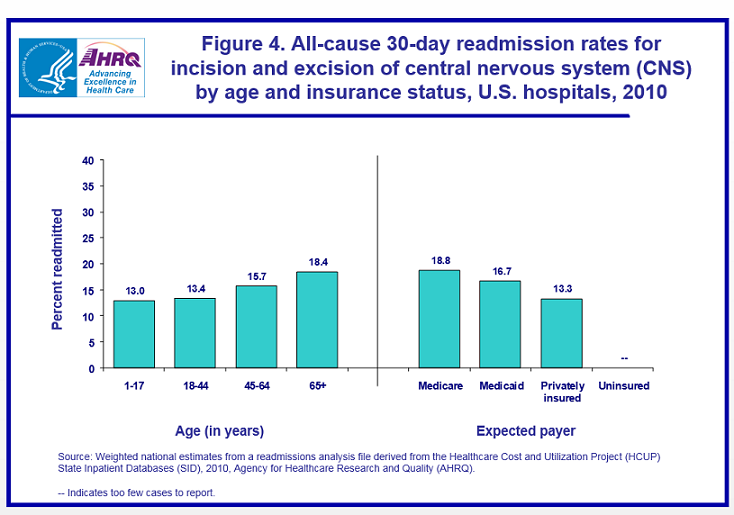
Readmission rates for incision and excision of the central nervous system (CNS) are depicted in figure 4. The highest readmission rate was for patients aged 65 years and older (18.4 percent), followed by patients aged 45–64 years (15.7 percent). Readmission rates were lowest and similar for the two youngest age groups (13.0–13.4 percent). Readmission rates were highest for patients covered by Medicare (18.8 percent), followed by Medicaid (16.7 percent) and private insurance (13.3 percent). |
|
Figure 4. All-cause 30-day readmission rates for incision and excision of central nervous system by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, 13.0 percent. Ages 18 through 44, 13.4 percent. Ages 45 through 64, 15.7 percent. Ages 65 and older, 18.4 percent. Medicare payer, 18.8 percent. Medicaid payer, 16.7 percent. Privately insured, 13.3 percent. Uninsured, too few cases to report. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
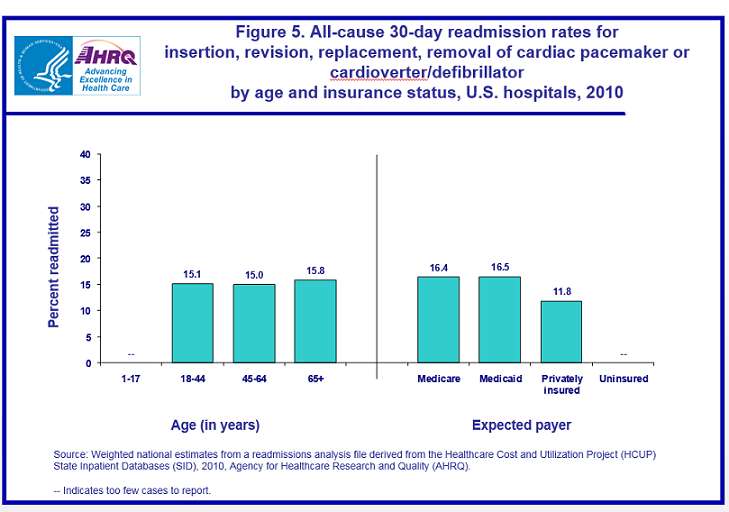
Figure 5 presents readmission rates for procedures related to a cardiac pacemaker or cardioverter/defibrillator. Readmission rates generally were similar for all adult age groups. Readmission rates were highest and similar for Medicare-covered (16.4 percent) and Medicaid-covered (16.5 percent) patients and lowest for privately insured patients (11.8 percent). |
|
Figure 5. All-cause 30-day readmission rates for insertion, revision, replacement, removal of cardiac pacemaker or cardioverter or defibrillator by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, too few cases to report. Ages 18 through 44, 15.1 percent. Ages 45 through 64, 15.0 percent. Ages 65 and older, 15.8 percent. Medicare payer, 16.4 percent. Medicaid payer, 16.5 percent. Privately insured, 11.8 percent. Uninsured, too few cases to report. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
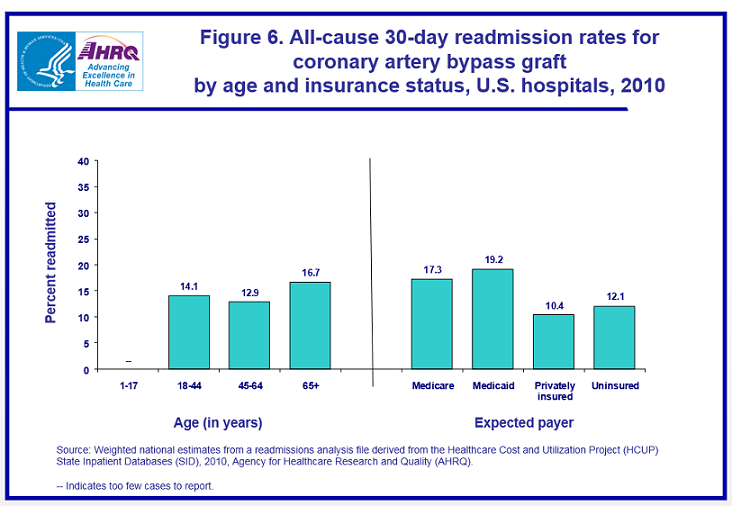
Finally, readmission rates for coronary artery bypass graft (CABG) are shown in figure 6. Readmission rates were highest for patients aged 65 years and older (16.7 percent), followed by those in age groups 18–44 (14.1 percent) and 45–64 (12.9 percent). The readmission rate was highest for patients with an expected payer of Medicaid (19.2 percent) or Medicare (17.3 percent) and lowest for the uninsured (12.1 percent) and those with private insurance (10.4 percent). |
|
Figure 6. All-cause 30-day readmission rates for coronary artery bypass graft by age and insurance status, U.S. hospitals, 2010. This is a bar chart showing percent readmitted by age in years and by expected payer. Ages 1 through 17, too few cases to report. Ages 18 through 44, 14.1 percent. Ages 45 through 64, 12.9 percent. Ages 65 and older, 16.7 percent. Medicare payer, 17.3 percent. Medicaid payer, 19.2 percent. Privately insured, 10.4 percent. Uninsured, 12.1 percent. Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project State Inpatient Databases, Agency for Healthcare Research and Quality.
|
Overall, across select procedures with high volume (more than 100,000 index stays) and high readmission rates (at least 15 percent), the 30-day readmission rate consistently was higher for patients aged 65 years and older than for younger adults. In terms of payer, patients with Medicare and Medicaid coverage also consistently had higher readmission rates than patients with private insurance or those who were uninsured. |
| Appendix. All-cause 30-day readmissions for selected procedures,* U.S. hospitals, 2010 | ||||
| All-listed procedure for index hospital stay (Clinical Classification Software procedure numbers and label/description) | Number of index stays | 30-day all-cause readmissions | ||
|---|---|---|---|---|
| Number of readmissions | Percent readmitted | |||
| Operations on the Nervous System | ||||
| 1 | Incision and excision of the central nervous system (CNS), (brain and spinal cord) | 105,700 | 17,019 | 16.1 |
| 2 | Insertion, replacement, or removal of extracranial ventricular shunt (passage to release spinal fluid) | 32,957 | 6,633 | 20.1 |
| 3 | Laminectomy, excision intervertebral disc (back surgery) | 456,664 | 30,383 | 6.7 |
| 5 | Insertion of catheter or spinal stimulator and injection into spinal canal | 6,302 | 637 | 10.1 |
| 6 | Decompression (removing pressure from) peripheral nerve | 15,834 | 1,436 | 9.1 |
| Operations on the Endocrine System | ||||
| 10 | Thyroidectomy, partial or complete (removal of all or part of thyroid gland) | 52,274 | 2,982 | 5.7 |
| Operations on the Ear, Nose, Mouth, and Phayrnx | ||||
| 23 | Myringotomy (tiny incision in the eardrum) | 8,777 | 764 | 8.7 |
| 28 | Plastic procedures on nose | 9,759 | 635 | 6.5 |
| Tonsillectomy and/or adenoidectomy (surgical removal of tonsil and/or adenoid) | 25,480 | 1,216 | 4.8 | |
| Operations on the Respiratory System | ||||
| 34 | Tracheostomy, temporary and permanent (surgical placement of a hole in the trachea—passage to lung—to assist breathing) | 9,335 | 2,234 | 23.9 |
| 36 | Lobectomy or pneumonectomy (surgical operation to remove an entire lung or part of a lung) | 82,264 | 9,431 | 11.5 |
| 37 | Diagnostic bronchoscopy and biopsy of bronchus (procedure to view and biopsy the breathing passages in the lung through a lighted tube) | 32,530 | 7,623 | 23.4 |
| 39 | Incision of pleura, thoracentesis, chest drainage (incision of lining of lungs, removal of fluid through a needle) | 13,933 | 2,648 | 19.0 |
| Operations on the Cardiovascular System | ||||
| 43 | Heart valve procedures | 110,615 | 20,502 | 18.5 |
| 44 | Coronary artery bypass graft (CABG), (procedure to restore blood supply to the heart muscle) | 234,840 | 35,484 | 15.1 |
| 45 | Percutaneous coronary angioplasty (PTCA), (procedure involving use of a balloon-tipped catheter to enlarge a narrowed artery) | 603,446 | 78,038 | 12.9 |
| 48 | Insertion, revision, replacement, removal of cardiac pacemaker or cardioverter/defibrillator | 149,147 | 23,057 | 15.5 |
| 51 | Endarterectomy, vessel of head and neck (surgical removal of an obstructing clot from the arteries of the neck and head) | 96,711 | 9,233 | 9.5 |
| 52 | Aortic resection, replacement or anastomosis (surgery on the great artery that carries blood to the body) | 46,861 | 6,116 | 13.1 |
| 55 | Peripheral vascular bypass (bypass of arteries in arms or legs to restore blood supply) | 72,529 | 15,005 | 20.7 |
| 57 | Procedures to create access for hemodialysis | 49,982 | 13,682 | 27.4 |
| 60 | Embolectomy and endarterectomy of lower limbs (surgical removal of an obstructing clot from the arteries of the legs) | 44,584 | 9,387 | 21.1 |
| Operations on the Hemic and Lymphatic System | ||||
| 64 | Bone marrow transplant | 19,919 | 2,905 | 22.5 |
| 66 | Procedures on spleen | 23,600 | 4,162 | 17.6 |
| Operations on the Digestive System | ||||
| 72 | Colostomy, temporary and permanent (surgical construction of an artificial anus between the colon and the surface of the abdomen that empties into a bag outside the body) | 46,675 | 8,859 | 19.0 |
| Ileostomy and other enterostomy (except colostomy), (surgical procedure where small intestine is attached to the abdominal wall and empties into a bag outside the body) | 23,392 | 6,811 | 29.1 | |
| 74 | Gastrectomy, partial and total (removal of all or part of the stomach) | 34,551 | 4,728 | 13.7 |
| 75 | Small bowel resection | 83,157 | 15,050 | 18.1 |
| 78 | Colorectal resection | 294,071 | 43,388 | 14.8 |
| 80 | Appendectomy (removal of appendix) | 315,034 | 18,835 | 6.0 |
| 81 | Hemorrhoid procedures | 9,298 | 1,020 | 11.0 |
| 83 | Biopsy of liver | 13,649 | 2,554 | 18.7 |
| 84 | Cholecystectomy (removal of gall bladder) and common duct exploration | 419,433 | 39,774 | 9.5 |
| 85 | Inguinal and femoral hernia repair | 38,067 | 3,632 | 9.5 |
| 87 | Laparoscopy (procedure in which a tiny scope is inserted into the abdomen through a small incision) | 59,918 | 6,570 | 11.0 |
| 89 | Exploratory laparotomy (abdominal surgery performed for diagnostic purposes) | 24,819 | 4,080 | 16.4 |
| 90 | Excision, lysis peritoneal adhesions | 342,425 | 42,126 | 12.3 |
| Operations on the Urinary System | ||||
| 100 | Endoscopy and endoscopic biopsy of the urinary tract (procedure to view and biopsy the urinary tract through a lighted tube) | 8,927 | 1,764 | 19.8 |
| 101 | Transurethral excision, drainage, or removal urinary obstruction | 88,139 | 11,795 | 13.4 |
| 103 | Nephrotomy and nephrostomy (procedure to establish an opening from the kidney to the exterior of the body) | 43,773 | 10,508 | 24.0 |
| 104 | Nephrectomy, partial or complete (surgical removal of kidney) | 61,905 | 5,881 | 9.5 |
| 105 | Kidney transplant | 16,761 | 4,882 | 29.1 |
| 106 | Genitourinary incontinence procedures | 78,767 | 2,327 | 3.0 |
| 109 | Procedures on the urethra (passage that carries urine from the bladder) | 11,062 | 1,083 | 9.8 |
| Operations on the Male Genital Organs | ||||
| 113 | Transurethral prostatectomy (TURP), (surgical removal of prostate gland through the urethra) | 59,777 | 5,509 | 9.2 |
| 114 | Open prostatectomy (surgery involving removal of part or all of the prostate gland) | 75,419 | 3,429 | 4.6 |
| Operations on the Female Genital Organs | ||||
| 119 | Oophorectomy, unilateral and bilateral (removal of an ovary or ovaries) | 288,228 | 17,480 | 6.1 |
| 121 | Ligation of fallopian tubes (for sterilization) | 238,190 | 4,819 | 2.0 |
| Obstetrical Procedures | ||||
| 124 | Hysterectomy, abdominal and vaginal (removal of the uterus) | 409,674 | 19,446 | 4.7 |
| 127 | Dilatation and curettage (D&C), aspiration after delivery or abortion | 26,335 | 736 | 2.8 |
| 128 | Diagnostic dilatation and curettage (D&C) | 14,851 | 1,537 | 10.4 |
| 129 | Repair of cystocele (bladder hernia) and rectocele (rectal hernia), obliteration of vaginal vault | 95,703 | 2,487 | 2.6 |
| 134 | Cesarean section (C-section) | 1,209,422 | 24,281 | 2.0 |
| Operations on the Musculoskeletal System | ||||
| 142 | Partial excision bone | 307,221 | 30,810 | 10.0 |
| 144 | Treatment, facial fracture or dislocation | 24,077 | 1,446 | 6.0 |
| 145 | Treatment, fracture or dislocation of radius and ulna (lower arm) | 57,263 | 3,616 | 6.3 |
| 146 | Treatment, fracture or dislocation of hip and femur | 278,118 | 33,049 | 11.9 |
| 147 | Treatment, fracture or dislocation of lower extremity (other than hip or femur) | 194,033 | 15,816 | 8.2 |
| 149 | Arthroscopy (procedure to view the inside of a joint through a lighted tube and to diagnose and treat problems) | 13,881 | 962 | 6.9 |
| 150 | Division of joint capsule, ligament or cartilage | 13,371 | 833 | 6.2 |
| 151 | Excision of semilunar cartilage of knee | 7,291 | 698 | 9.6 |
| 152 | Arthroplasty knee (surgical reconstruction or replacement of knee) | 651,965 | 32,764 | 5.0 |
| 153 | Hip replacement, total and partial | 424,408 | 34,265 | 8.1 |
| 154 | Arthroplasty other than hip or knee (surgical reconstruction or replacement of other joints) | 76,498 | 3,926 | 5.1 |
| 157 | Amputation of lower extremity (leg, foot, or toe) | 124,880 | 28,488 | 22.8 |
| 158 | Spinal fusion (correction of an unstable part of the spine by joining two or more vertebrae) | 431,577 | 29,326 | 6.8 |
| Operations on the Integumentary System and Breast | ||||
| 166 | Lumpectomy, quadrantectomy of breast (operation to remove a lump from the breast) | 12,872 | 1,095 | 8.5 |
| 167 | Mastectomy (operation to remove the whole breast) | 61,885 | 3,868 | 6.3 |
| 169 | Debridement of wound, infection or burn (surgical removal of foreign material and dead tissue from a wound, infection or burn) | 148,544 | 28,394 | 19.1 |
| 170 | Excision of skin lesion | 7,404 | 1,007 | 13.6 |
| 172 | Skin graft (procedure during which a piece of skin is taken from a donor area and surgically grafted at the site of an injury or burn) | 97,756 | 14,789 | 15.1 |
| Miscellaneous Diagnostic and Therapeutic Procedures | ||||
| 184 | Intraoperative cholangiogram (X-ray procedure where a contrast dye is injected into the bile duct during surgery) | 134,934 | 11,551 | 8.6 |
| 211 | Therapeutic radiology | 5,183 | 1,212 | 23.4 |
| Source: Weighted national estimates from a readmissions analysis file derived from the Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID), 2010, Agency for Healthcare Research and Quality (AHRQ). * Information is provided for procedures with at least 5,000 weighted occurrences and 500 or more weighted readmissions. See text and Definitions for details on methods for calculating readmissions. |
||||
Data Source
The estimates in this Statistical Brief are based on a readmissions analysis file that was created with the Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID). These databases include reliable, verified synthetic patient identifiers that can be used to track a person across hospitals within a State. Estimates were taken from HCUPnet, the online query system that provides free access to information from HCUP: https://datatools.ahrq.gov/hcupnet. HCUPnet provides access to health statistics and information on hospital inpatient and emergency department utilization, and it includes analytic tables using the readmissions analysis file. HCUPnet contains additional detailed results and sortable tables that provide instant information on readmissions to the hospital within 30 days of discharge. For 2010, readmissions data were available from 18 States: Alaska, Arkansas, California, Florida, Georgia, Hawaii, Louisiana, Massachusetts, Mississippi, Missouri, Nebraska, New Mexico, New York, South Carolina, Tennessee, Utah, Virginia, and Washington. These 18 States are geographically dispersed and account for 46 percent of the total U.S. resident population and 45 percent of the total U.S. hospitalizations. The readmissions analysis file included 14.0 million unweighted discharges. The study population in this readmissions analysis file included discharges from community, nonrehabilitation, nonspecialty hospitals. Weights for national estimates were developed using poststratification on hospital characteristics (Census region, urban-rural location, teaching capabilities, bed size, and control/ownership) and patient age groups. Definitions Procedures, ICD-9-CM, and Clinical Classifications Software (CCS) All-listed procedures include all procedures performed during the hospital stay whether for definitive treatment or for diagnostic or exploratory purposes. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to procedures. There are approximately 4,000 ICD-9-CM procedure codes. CCS categorizes procedure codes into clinically meaningful categories.9 This "clinical grouper" makes it easier to quickly understand patterns of procedure use. CCS categories identified as "Other" typically are not reported; these categories include miscellaneous, otherwise unclassifiable procedures that may be difficult to interpret as a group. Readmissions The 30-day readmission rate is defined as the number of admissions for each procedure for which there was at least one subsequent hospital admission within 30 days, divided by the total number of admissions from January through November 2010. That is, when patients are discharged from the hospital, they are followed for 30 days in the data. If any readmission to the same or different hospital occurs during this time period, the admission is counted as a readmission. No more than one readmission is counted within the 30-day period, because the outcome measure assessed is "percentage of admissions who are readmitted." If a patient was transferred to a different hospital on the same day or was transferred within the same hospital, the two events were combined as a single stay and the second event was not counted as a readmission; that is, transfers were not considered a readmission. In the case of admissions for which there was more than one readmission in the 30-day period, the data presented in this Statistical Brief reflect the characteristics and costs of the first readmission. Every qualifying hospital stay is counted as a separate index (starting point) admission. Thus, a single patient can be counted multiple times during the course of the January through November observation period. In addition, index admissions do not require a prior "clean period" with no hospitalizations; that is, a hospital stay may be a readmission for a prior stay and the index admission for a subsequent readmission. Admissions were disqualified from the analysis as index admissions if they could not be followed for 30 days for one of the following reasons: (1) admissions in which the patient died in the hospital, (2) admissions missing information on length of stay, and (3) admissions discharged in December 2010. Types of hospitals included in HCUP HCUP is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). HCUP data include obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care, rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Payer (Insurance Status) Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into more general groups:
About HCUP HCUP is a family of powerful healthcare databases, software tools, and products for advancing research. Sponsored by the Agency for Healthcare Research and Quality (AHRQ), HCUP includes the largest all-payer encounter-level collection of longitudinal healthcare data (inpatient, ambulatory surgery, and emergency department) in the United States, beginning in 1988. HCUP is a Federal-State-Industry Partnership that brings together the data collection efforts of many organizations—such as State data organizations, hospital associations, private data organizations, and the Federal government—to create a national information resource. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health and Hospitals Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Health Policy and Research Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Budget & Control Board South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the SID The HCUP State Inpatient Databases (SID) are hospital inpatient databases from data organizations participating in HCUP. The SID contain the universe of the inpatient discharge abstracts in the participating HCUP States, translated into a uniform format to facilitate multistate comparisons and analyses. Together, the SID encompass more than 95 of all U.S. community hospital discharges in 2010. The SID can be used to investigate questions unique to one State, to compare data from two or more States, to conduct market area variation analyses, and to identify State-specific trends in inpatient care utilization, access, charges, and outcomes. About HCUPnet HCUPnet is an online query system that offers instant access to the largest set of all-payer healthcare databases publicly available. HCUPnet has an easy step-by-step query system, allowing for tables and graphs to be generated on national and regional statistics as well as trends for community hospitals in the United States. HCUPnet generates statistics using data from HCUP's Nationwide Inpatient Sample (NIS), the Kids' Inpatient Database (KID), the Nationwide Emergency Department Sample (NEDS), the State Inpatient Databases (SID), and the State Emergency Department Databases (SEDD). For More Information For more information about HCUP, visit http://www.hcup-us.ahrq.gov/. For additional HCUP statistics, visit HCUPnet, our interactive query system, at https://datatools.ahrq.gov/hcupnet. HCUPnet provides ready-to-use tables on readmission rates by condition and procedure (using Clinical Classification Software categories), diagnosis related groups (DRGs), and major diagnostic categories (MDCs). Suggested Citation Weiss AJ (Truven Health Analytics), Elixhauser A (AHRQ), Steiner C (AHRQ). Readmissions to U.S. Hospitals by Procedure, 2010. HCUP Statistical Brief #154. April 2013. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb154.pdf. Acknowledgements The authors would like to acknowledge the contributions of Marguerite Barrett and Minya Sheng for work on programming. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Irene Fraser, Ph.D., Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 540 Gaither Road Rockville, MD 20850 1 Stone J, Hoffman GJ. Medicare Hospital Readmissions: Issues, Policy Options and PPACA. 2010. Congressional Research Service Report for Congress. www.everycrsreport.com/files/20100921_R40972_fc06768f2d6d1230fa436de550b1bd8db82bd644.pdf. 2 Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare Fee-for-Service Program. N Engl J Med. 2009;360:1418-28. 3Public Law 111-148, Patient Protection and Affordable Care Act 2010: Part III, Section 33025. March 2010. http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf. Accessed April 3, 2013. 4 Kassin MT, Owen RM, Perez SD, et al. Risk factors for 30-day hospital readmission among general surgery patients. J Am Coll Surg. 2012;215:322-30. 5 Goodney PP, Stukel TA, Lucas FL, et al. Hospital volume, length of stay, and readmission rates in high-risk surgery. Ann Surg. 2003;238:161-7. 6 Khawaja FJ, Shah ND, Lennon RJ, et al. Factors associated with 30-day readmission rates after percutaneous coronary intervention. Arch Intern Med. 2012;172:112-7. 7 Meadows ES, Bae JP, Zagar A, et al. Rehospitalization following percutaneous coronary intervention for commercially insured patients with acute coronary syndrome: A retrospective analysis. BMC Research Notes. 2012;5:342. http://www.biomedcentral.com/1756-0500/5/342. 8 https://datatools.ahrq.gov/hcupnet 9 HCUP Clinical Classifications Software (CCS). Healthcare Cost and Utilization Project (HCUP). U.S. Agency for Healthcare Research and Quality, Rockville, MD. Updated March 2013. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed April 3, 2013. |