STATISTICAL BRIEF #206 |
June 2016
Kevin C. Heslin, Ph.D., and Anne Elixhauser, Ph.D. Introduction Human immunodeficiency virus (HIV) is a global health problem, causing over 34 million deaths since the virus was first identified in the early 1980s. In the United States, approximately 675,000 people with HIV have died.1 Currently, 1.2 million people in the United States are living with HIV, and an estimated 50,000 new infections occur each year.2 Since 1996, the availability of combination antiretroviral therapy to suppress the virus has allowed more people with HIV to live healthier and longer lives. By mid-2015, over 15 million people worldwide were receiving these medications.3 Between 2000 and 2015, new HIV infections decreased worldwide by 35 percent and HIV-related deaths decreased by 24 percent.4 These improvements in care are helping to transform HIV disease from a rapidly fatal illness to a chronic condition—leading, in turn, to the growth of an aging HIV-positive population. By 2020, it is expected that the majority of people with HIV disease in the United States will be aged 50 years or older—compared with 2009, when only one-third of people with HIV were that age.5 Access to medications for HIV disease has been supported by a number of health policies and programs. Since 1990, the Ryan White Program has served as a "payer of last resort" for people with HIV who are under- or uninsured, providing HIV medications to people with minimal or no prescription drug coverage through the AIDS Drug Assistance Programs in all 50 states.6 Historically, Medicaid has been the most common source of coverage for people with HIV, and the 2010 Patient Protection and Affordable Care Act called for expanding Medicaid to nearly all adults with incomes of up to 138 percent of the Federal Poverty Level. In June 2012, the U.S. Supreme Court ruled that States could decide whether to participate in the Patient Protection and Affordable Care Act Medicaid expansion. In States that have expanded Medicaid, previously uninsured people with HIV who were not eligible through the traditional income and disability criteria of the Social Security Income program have obtained coverage. A recent analysis using six Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases found that the percentage of uninsured hospital stays among HIV patients fell from 13.7 percent to 5.5 percent between 2012 through 2014 in four Medicaid expansion States, while increasing from 14.5 percent to 15.7 percent in two comparison States that did not expand Medicaid. |
|
The Patient Protection and Affordable Care Act will eliminate the gap in prescription drug coverage (the "donut hole") in Medicare Part D by 2020, which will reduce copayments on expensive medications for Medicare beneficiaries with HIV. For people who are not eligible for Medicaid or Medicare, the Patient Protection and Affordable Care Act has increased access to private insurance through the State health insurance exchanges that were introduced in late 2014. Insurance plans offered on the exchanges must cover an essential benefits package and cannot include lifetime or annual coverage caps or provisions that limit coverage for pre-existing conditions such as HIV disease.
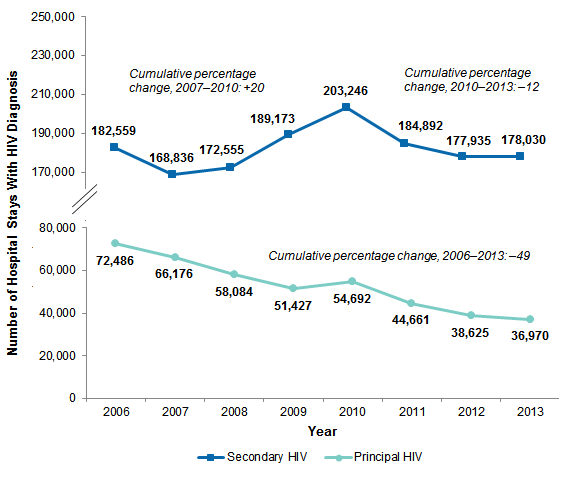
Despite the progress that has been made in available treatments and coverage expansions, it has been estimated that only 25 percent of people with HIV disease in the United States achieve the viral suppression necessary to maintain long-term health.9 People with HIV disease continue to experience opportunistic infections, cancers, and other serious conditions more often than do demographically similar people without HIV. Historically, the most common HIV-related opportunistic infections have been pneumocystis pneumonia and esophageal candidiasis.10 Other opportunistic infections that rarely occur in patients with intact immune systems include those caused by organisms such as mycobacteria, cryptococcus, and cytomegalovirus. Cancers related to HIV include Kaposi's sarcoma, primary cerebral lymphoma, and non-Hodgkin's lymphoma.11 Because people with HIV disease are living longer, noninfectious complications and comorbid diseases have increased in frequency.12 Antiretroviral therapy for HIV also involves side effects and long-term toxicities, which may occur more frequently in older patients who have greater risks of pharmacological interactions with non-HIV medications. Antiretroviral therapy is associated with disorders of lipid metabolism.13 By accelerating atherosclerosis, HIV medications may also increase the risk of hypertension and stroke.14 These conditions contribute to disability and mortality among people with HIV disease, and their treatment often involves hospitalization. This HCUP Statistical Brief updates a previous Brief on hospital stays that included diagnoses of HIV disease from 1998 through 2005.15 The current Brief presents data from the National (Nationwide) Inpatient Sample from the 2006-2013 period to examine trends in hospital stays that include principal and secondary diagnoses of HIV, as well as age-specific trends in hospitalization rates per 100,000 population. Differences of 10 percent or greater are noted in the text. As in the previous Statistical Brief on HIV hospitalizations, we report on major HIV-related conditions that usually do not occur in people whose immune systems are not compromised. These conditions are cited in the 2014 HIV infection surveillance case definition by the Centers for Disease Control and Prevention.16 Finally, we provide information on the 15 most common diagnoses (principal and secondary) among stays that include any diagnosis of HIV disease for 2006, 2010, and 2013. Findings Changes in hospital stays that involve HIV disease, 2006-2013 Figure 1 presents the number of hospital stays that included a principal diagnosis of HIV disease, as well as the number of stays with a secondary HIV diagnosis, for each year between 2006 and 2013. |
|
Figure 1. Hospital stays including a principal or secondary diagnosis of HIV, 2006-2013
Abbreviation: HIV, human immunodeficiency virus Figure 1 is a line graph that shows the number of hospital stays with a principal or secondary HIV diagnosis by year. For principal HIV diagnoses, the number of hospital stays was: 2006: 72,486; 2007: 66,176; 2008: 58,084; 2009: 51,427; 2010: 54,692; 2011: 44,661; 2012: 38,625; 2013: 36,970. The cumulative percentage change for 2006-2013 was -49%. For secondary HIV diagnoses, the number of hospital stays was: 2006: 182,559; 2007: 168,836; 2008: 172,555; 2009: 189,173; 2010: 203,246; 2011: 184,892; 2012: 177,935; 2013: 178,030. The cumulative percentage change for 2007-2010 was 20% and for 2010-2013 was -12%.
|
|
|
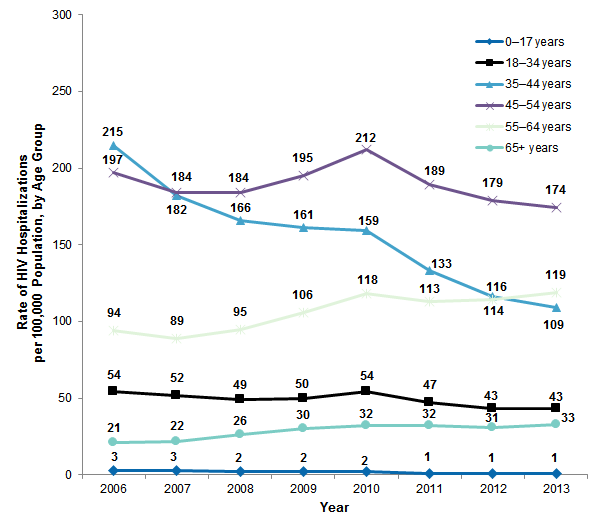
Figure 2. Rate of hospital inpatient stays including HIV per 100,000 population by age group, 2006-2013
Abbreviation: HIV, human immunodeficiency virus Figure 2 is a line graph that shows the rate of HIV hospitalizations per 100,000 population by age group by year. 0-17 years: 2006: 3; 2007: 3; 2008: 2; 2009: 2; 2010: 2; 2011: 1; 2012: 1; 2013: 1. 18-34 years: 2006: 54; 2007: 52; 2008: 49; 2009: 50; 2010: 54; 2011: 47; 2012: 43; 2013: 43. 35-44 years: 2006: 215; 2007: 182; 2008: 166; 2009: 161; 2010: 159; 2011: 133; 2012: 116; 2013: 109. 45-54 years: 2006: 197; 2007: 184; 2008: 184; 2009: 195; 2010: 212; 2011: 189; 2012: 179; 2013: 174. 55-64 years: 2006: 94; 2007: 89; 2008: 95; 2009: 106; 2010: 118; 2011: 113; 2012: 114; 2013: 119. 65+ years: 2006: 21; 2007: 22; 2008: 26; 2009: 30; 2010: 32; 2011: 32; 2012: 31; 2013: 33.
|
For 2006, 2010, and 2013, Table 1 presents stays with a principal or secondary HIV diagnosis by patient characteristics and resource use, as well as the cumulative percentage change between 2006 and 2013. |
| Table 1. National estimates of hospital stays that included an HIV diagnosis, 2006, 2010, and 2013 | |||||||
| Characteristic/Outcome | 2006 | 2010 | 2013 | Percent change, 2006-2013 | |||
|---|---|---|---|---|---|---|---|
| Number of stays | % of stays | Number of stays | % of stays | Number of stays | % of stays | ||
| Total stays (all-listed) | 255,035 | 100.0 | 257,938 | 100.0 | 215,000 | 100.0 | -16 |
| Died during inpatient stay | 8,357 | 3.3 | 7,689 | 3.0 | 5,400 | 2.5 | -35 |
| Patient characteristics | |||||||
| Sex | |||||||
| Female | 88,511 | 34.7 | 90,191 | 35.0 | 73,110 | 34.0 | -17 |
| Male | 166,524 | 65.3 | 167,737 | 65.0 | 141,860 | 66.0 | -15 |
| Payer | |||||||
| Medicare | 69,424 | 27.2 | 74,319 | 28.9 | 71,770 | 33.4 | 3 |
| Medicaid | 108,356 | 42.5 | 106,464 | 41.5 | 81,965 | 38.2 | -24 |
| Private | 39,450 | 15.5 | 37,182 | 14.5 | 34,070 | 15.9 | -14 |
| Other | 11,095 | 4.4 | 8,124 | 3.2 | 6,955 | 3.2 | -37 |
| Uninsured | 26,522 | 10.4 | 30,741 | 12.0 | 19,965 | 9.3 | -25 |
| HIV-related conditionsa | |||||||
| Cytomegaloviral disease | 3,699 | 1.5 | 3,938 | 1.5 | 3,195 | 1.5 | -14 |
| Mycobacterial disease | 5,561 | 2.2 | 4,926 | 1.9 | 3,450 | 1.6 | -38 |
| Toxoplasmosis | 3,356 | 1.3 | 2,921 | 1.1 | 1,515 | 0.7 | -55 |
| Pneumocystosis | 13,611 | 5.3 | 10,870 | 4.2 | 7,790 | 3.6 | -43 |
| Pulmonary tuberculosis | 1,768 | 0.7 | 1,308 | 0.5 | 780 | 0.4 | -56 |
| Candidiasis | 34,586 | 13.6 | 30,313 | 11.8 | 21,865 | 10.2 | -37 |
| Kaposi's sarcoma | 2,991 | 1.2 | 3,242 | 1.3 | 2,500 | 1.2 | -16 |
| History of recurrent pneumoniab | 1,003 | 0.4 | 2,596 | 1.0 | 2,535 | 1.2 | 153 |
| Weight loss | 2,536 | 1.0 | 4,833 | 1.9 | 5,000 | 2.3 | 97 |
| Mean | Mean | Mean | |||||
| Resource use | |||||||
| Length of stay, mean days | 6.8 | 6.5 | 6.1 | -10 | |||
| Inflation-adjusted cost per stay, mean, U.S. $c | 12,589 | 12,719 | 13,300 | 6 | |||
| Inflation-adjusted hospital costs, total, $ billionsc | 3.20 | 3.9 | 2.83 | -12 | |||
| Abbreviations: HIV, human immunodeficiency virus a The list of HIV-related conditions is taken from Selik RM, Mokotoff ED, Branson B, Owen SM, Whitmore S, Hall HI. Revised Surveillance Case Definition for HIV Infection-United States, 2014. MMWR. 2014;63(3):1-10. b This diagnosis is based on a “V code” that specifically indicates a personal history of recurrent pneumonia and may not necessarily indicate active pneumonia during the hospital stay. c Costs in 2006 and 2010 were adjusted for inflation to the 2013 level using Gross Domestic Product price indices for those years. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Inpatient Sample (NIS) 2006-2011, National Inpatient Sample (NIS), 2012-2013 | |||||||
|
| Table 2. Fifteen most common all-listed diagnoses (principal or secondary) for HIV hospital stays in 2006, 2010, and 2013 | |||||||||
| Rank | All-listed diagnoses, 2006 | Number of stays | % of stays | All-listed diagnoses, 2010 | Number of stays | % of stays | All-listed diagnoses, 2013 | Number of stays | % of stays |
|---|---|---|---|---|---|---|---|---|---|
| 1 | HIV disease | 255,035 | 100.0 | HIV disease | 257,938 | 100.0 | HIV disease | 215,000 | 100.0 |
| 2 | Hypertension | 76,318 | 29.9 | Hypertension | 97,595 | 37.8 | Hypertension | 93,555 | 43.5 |
| 3 | Substance-related disorders | 72,527 | 28.4 | Screening and history of mental health and substance abuse codes | 87,675 | 34.0 | Screening and history of mental health and substance abuse codes | 86,945 | 40.4 |
| 4 | Fluid and electrolyte disorders | 67,828 | 26.6 | Deficiency and other anemia | 77,974 | 30.2 | Fluid and electrolyte disorders | 72,125 | 33.6 |
| 5 | Deficiency and other anemia | 66,129 | 25.9 | Fluid and electrolyte disorders | 76,740 | 29.8 | Deficiency and other anemia | 69,850 | 32.5 |
| 6 | Screening and history of mental health and substance abuse codes | 61,668 | 24.2 | Substance-related disorders | 64,040 | 24.8 | Renal failure | 59,640 | 27.7 |
| 7 | Hepatitis | 51,618 | 20.2 | Hepatitis | 60,493 | 23.5 | Asthma and COPD | 54,405 | 25.3 |
| 8 | Pneumonia | 50,326 | 19.7 | Asthma and COPD | 59,885 | 23.2 | Mood disorders | 55,245 | 25.7 |
| 9 | Asthma and COPD | 49,950 | 19.6 | Renal failure | 59,084 | 22.9 | Substance-related disorders | 52,705 | 24.5 |
| 10 | Mood disorders | 47,070 | 18.5 | Mood disorders | 57,963 | 22.5 | Hepatitis | 47,785 | 22.2 |
| 11 | Renal failure | 42,949 | 16.8 | Pneumonia | 46,306 | 18.0 | Diabetes | 40,330 | 18.8 |
| 12 | Mycoses | 40,859 | 16.0 | Diabetes | 42,312 | 16.4 | Pneumonia | 36,660 | 17.1 |
| 13 | Alcohol-related disorders | 32,967 | 12.9 | Mycoses | 35,697 | 13.8 | Disorders of lipid metabolism | 32,930 | 15.3 |
| 14 | Diabetes | 32,203 | 12.6 | Alcohol-related disorders | 32,837 | 12.7 | Nutritional deficiencies | 27,750 | 12.8 |
| 15 | Bacterial infections, unspecified | 24,079 | 9.4 | Nutritional deficiencies | 27,530 | 0.7 | Mycoses | 25,175 | 11.7 |
| Abbreviation: COPD, chronic obstructive pulmonary disease; HIV, human immunodeficiency virus Note: Diagnoses were identified using AHRQ's Clinical Classifications Software (CCS). Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Inpatient Sample (NIS) 2006-2011, National Inpatient Sample (NIS), 2012-2013 | |||||||||
Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) for 2012 and 2013 and the Nationwide Inpatient Sample (NIS) for 2006-2011. Supplemental sources included population denominator data for use with HCUP databases, derived from information available from the Bureau of the Census.17 Definitions Diagnoses, ICD-9-CM, Clinical Classifications Software (CCS) The principal diagnosis is the condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses. There are approximately 14,000 ICD-9-CM diagnosis codes. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.18 This clinical grouper makes it easier to quickly understand patterns of diagnoses. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. Case definition In this report, a hospital stay was designated as including HIV disease if the relevant CCS code for HIV (i.e., CCS #5: ICD-9-CM codes: 042 0420 0421 0422 0429 0430 0431 0432 0433 0439 0440 0449 07953 27910 27919 79571 7958 V08) appeared as any all-listed diagnosis on the patient record. The ICD-9-CM diagnosis codes used to define HIV-related conditions are listed in Table 3. |
| Table 3. ICD-9-CM diagnosis codes defining HIV-related conditions | |
| ICD-9-CM code | Definition |
|---|---|
| Cytomegaloviral disease | |
| 078.5 | Cytomegaloviral disease |
| Mycobacterial disease | |
| 031.0 | Pulmonary mycobacterial disease |
| 031.1 | Cutaneous mycobacterial disease |
| 031.2 | Disseminated mycobacterial disease |
| 031.8 | Disseminated mycobacterial disease |
| 031.9 | Unspecified diseases due to mycobacteria |
| Toxoplasmosis | |
| 130.0 | Meningoencephalitis due to toxoplasmosis |
| 130.1 | Conjunctivitis due to toxoplasmosis |
| 130.2 | Chorioretinitis due to toxoplasmosis |
| 130.3 | Myocarditis due to toxoplasmosis |
| 130.4 | Pneumonitis due to toxoplasmosis |
| 130.5 | Hepatitis due to toxoplasmosis |
| 130.7 | Toxoplasmosis of other specified sites |
| 130.8 | Multisystemic disseminated toxoplasmosis |
| 130.9 | Toxoplasmosis, unspecified |
| Pneumocystosis | |
| 136.3 | Pneumocystosis |
| Pulmonary tuberculosis | |
| 011.0 | Tuberculosis of lung, infiltrative |
| 011.1 | Tuberculosis of lung, nodular |
| 011.2 | Tuberculosis of lung with cavitation |
| 011.3 | Tuberculosis of bronchus |
| 011.4 | Tuberculous fibrosis of lung |
| 011.5 | Tuberculous bronchiectasis |
| 011.6 | Tuberculous pneumonia |
| 011.7 | Tuberculous pneumothorax |
| 011.8 | Other specified pulmonary tuberculosis |
| 011.9 | Pulmonary tuberculosis, unspecified |
| Candidiasis | |
| 112.0 | Candidiasis of mouth |
| 112.1 | Candidiasis of vulva and vagina |
| 112.2 | Candidiasis of urogenital sites |
| 112.3 | Candidiasis of skin and nails |
| 112.4 | Candidiasis of lung |
| 112.5 | Candidiasis, disseminated |
| 112.8 | Candidiasis of other specified sites |
| 112.9 | Candidiasis of unspecified site |
| Kaposi's sarcoma | |
| 176.0 | Kaposi's sarcoma, skin |
| 176.1 | Kaposi's sarcoma, soft tissue |
| 176.2 | Kaposi's sarcoma, palate |
| 176.3 | Kaposi's sarcoma, gastrointestinal sites |
| 176.4 | Kaposi's sarcoma, lung |
| 176.5 | Kaposi's sarcoma, lymph nodes |
| 176.8 | Kaposi's sarcoma, other specified sites |
| 176.9 | Kaposi's sarcoma, unspecified |
| History of recurrent pneumonia | |
| V12.61 | Personal history of recurrent pneumonia |
| Weight loss | |
| 783.21 | Loss of weight |
| 783.22 | Underweight |
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Costs and charges Total hospital charges were converted to costs using HCUP Cost-to-Charge Ratios based on hospital accounting reports from the Centers for Medicare & Medicaid Services (CMS).19 Costs reflect the actual expenses incurred in the production of hospital services, such as wages, supplies, and utility costs; charges represent the amount a hospital billed for the case. For each hospital, a hospital-wide cost-to-charge ratio is used. Hospital charges reflect the amount the hospital billed for the entire hospital stay and do not include professional (physician) fees. n 1 year will be counted each time as a separate discharge from the hospital. In this Statistical Brief, costs in 2006 and 2010 are adjusted for inflation to the 2013 level using the Gross Domestic Product (GDP) Price Index from the U.S. Department of Commerce, Bureau of Economic Analysis (BEA) for those years.20 That is, all costs are expressed in 2013 dollars. Mean cost per day is calculated as the cost per stay divided by the length of stay and is reported to the nearest hundred. How HCUP estimates of costs differ from National Health Expenditure Accounts There are a number of differences between the costs cited in this Statistical Brief and spending as measured in the National Health Expenditure Accounts (NHEA), which are produced annually by CMS.21 The largest source of difference comes from the HCUP coverage of inpatient treatment only in contrast to the NHEA inclusion of outpatient costs associated with emergency departments and other hospital-based outpatient clinics and departments as well. The outpatient portion of hospitals' activities has been growing steadily and may exceed half of all hospital revenue in recent years. On the basis of the American Hospital Association Annual Survey, 2012 outpatient gross revenues (or charges) were about 44 percent of total hospital gross revenues.22 Smaller sources of differences come from the inclusion in the NHEA of hospitals that are excluded from HCUP. These include Federal hospitals (Department of Defense, Veterans Administration, Indian Health Services, and Department of Justice [prison] hospitals) as well as psychiatric, substance abuse, and long-term care hospitals. A third source of difference lies in the HCUP reliance on billed charges from hospitals to payers, adjusted to provide estimates of costs using hospital-wide cost-to-charge ratios, in contrast to the NHEA measurement of spending or revenue. HCUP costs estimate the amount of money required to produce hospital services, including expenses for wages, salaries, and benefits paid to staff as well as utilities, maintenance, and other similar expenses required to run a hospital. NHEA spending or revenue measures the amount of income received by the hospital for treatment and other services provided, including payments by insurers, patients, or government programs. The difference between revenues and costs include profit for for-profit hospitals or surpluses for nonprofit hospitals. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
Hospital stays billed to the State Children's Health Insurance Program (SCHIP) may be classified as Medicaid, Private Insurance, or Other, depending on the structure of the State program. Because most State data do not identify patients in SCHIP specifically, it is not possible to present this information separately. For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health and Hospitals Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About Statistical Briefs HCUP Statistical Briefs are descriptive summary reports presenting statistics on hospital inpatient and emergency department use and costs, quality of care, access to care, medical conditions, procedures, patient populations, and other topics. The reports use HCUP administrative healthcare data. About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
For More Information For more information about HCUP, visit http://www.hcup-us.ahrq.gov/. For additional HCUP statistics, visit HCUP Fast Stats at https://datatools.ahrq.gov/hcup-fast-stats for easy access to the latest HCUP-based statistics for health information topics, or visit HCUPnet, our interactive query system, at https://datatools.ahrq.gov/hcupnet. For information on other HIV hospitalizations in the United States, refer to the following HCUP Statistical Brief located at http://www.hcup-us.ahrq.gov/reports/statbriefs/statbriefs.jsp:
For a detailed description of HCUP and more information on the design of the National (nationwide) Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2015. http://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 17, 2016. Suggested Citation Heslin KC (AHRQ), Elixhauser A (AHRQ). HIV Hospital Stays in the United States, 2006-2013. HCUP Statistical Brief #206. June 2016. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb206-HIV-Hospital-Stays-Trends.pdf. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:David Knutson, Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 1 Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas, 2014. HIV Surveillance Report, Vol. 26. November 2015. www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2014-vol-26.pdf. Accessed October 27, 2021. 2 Centers for Disease Control and Prevention. HIV in the United States: At a Glance. 2015. http://www.cdc.gov/hiv/statistics/overview/ataglance.html. Accessed January 25, 2016. 3 UNAIDS. 15 by 15: A Global Target Achieved. Geneva, Switzerland: UNAIDS; 2015. 4 World Health Organization (WHO). HIV/AIDS. Fact Sheet #360. Updated November 2015. http://www.who.int/mediacentre/factsheets/fs360/en/. 5 Goldman TR. Living with HIV and growing old. Health Affairs. 2014;33:3:359-61 6 Kaiser Family Foundation. The Ryan White Program. Menlo Park, CA: Kaiser Family Foundation; March 2013. http://kff.org/hivaids/fact-sheet/the-ryan-white-program/ 7 Kates J. How the ACA changes pathways to insurance coverage for people with HIV. Menlo Park, CA: Kaiser Family Foundation; September 18, 2012. http://kff.org/hivaids/perspective/how-the-aca-changes-pathways-to-insurance-coverage-for-people-with-hiv/. 8 Hellinger FJ. In four ACA expansion States, the percentage of uninsured hospitalizations for people with HIV declined, 2012-2014. Health Affairs. 2015;34(12):2061-8. 9 Hall HI, Frazier EL, Rhodes P, Holtgrave DR, Furlow-Parmley C, Tang T, et al. Differences in human immunodeficiency virus care and treatment among subpopulations in the United States. Journal of the American Medical Association. 2013;173(14):1337-44. 10 Beers MH, Jones TV. Human Immunodeficiency Virus Infection. In: The Merck Manual of Geriatrics, 3rd ed. Whitehouse Station, NJ: Merck Research Laboratories; 2005:1378-82. 11 Sterling TR, Chaisson RE. General Clinical Manifestations of Human Immunodeficiency Virus Infection. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2004:1546-66. 12 Crum NF, Riffenburgh RH, Wegner S, Agan BK, Tasker SA, Spooner KM, et al. Comparisons of causes of death and mortality rates among HIV-infected persons: analysis of the pre-, early, and late HAART (highly active antiretroviral therapy) eras. Journal of the Acquired Immune Deficiency Syndromes. 2006;41:194-200. 13 Wohl DA. Considering metabolic issues when initiating HIV therapy. Current HIV/AIDS Reports. 2007;4(3):119-25. 14 Benjamin LA, Bryer A, Emsley HC, Khoo S, Solomon T, Connor MD. HIV infection and stroke: current perspectives and future directions. Lancet Neurology. 2012;11(10):878-90. 15 Zhao Y, Encinosa W, Hellinger F. HIV Hospitalizations in 1998 and 2005. HCUP Statistical Brief #41. November 2007. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb41.pdf. 16 Selik RM, Mokotoff ED, Branson B, Owen SM, Whitmore S, Hall HI. Revised Surveillance Case Definition for HIV Infection-United States, 2014. MMWR. 2014;63(3):1-10. 17 Barrett M, Hickey K, Coffey R, Levit K. Population Denominator Data for Use with the HCUP Databases (Updated with 2014 Population Data). HCUP Methods Series Report #2015-07. September 1, 2015. U.S. Agency for Healthcare Research and Quality. hhttp://www.hcup-us.ahrq.gov/reports/methods/2015-07.pdf. Accessed February 17, 2016. 18 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated June 2015. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed February 17, 2016. 19 Agency for Healthcare Research and Quality. HCUP Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). 2001-2012. Rockville, MD: Agency for Healthcare Research and Quality. Updated December 2014. http://www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed February 17, 2016. 20 U.S. Bureau of Economic Analysis. National Income and Product Account Tables, Table 1.1.4 Price Indexes for Gross Domestic Product. http://www.bea.gov/iTable/iTable.cfm?ReqID=9&step=1#reqid=9&step=1&isuri=1. Accessed February 17, 2016. 21 For additional information about the NHEA, see Centers for Medicare & Medicaid Services (CMS). National Health Expenditure Data. CMS website May 2014. http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/index.html?redirect=/NationalHealthExpendData/. Accessed February 17, 2016. 22 American Hospital Association. TrendWatch Chartbook, 2014. Table 4.2. Distribution of Inpatient vs. Outpatient Revenues, 1992-2012. Original source is no longer available on the Web; for related information refer to TrendWatch Chartbook, 2018. Table 4.2. Distribution of Inpatient vs. Outpatient Revenues, 1995-2016. www.aha.org/system/files/2018-05/2018-chartbook-table-4-2.pdf. |
| Internet Citation: Statistical Brief #206. Healthcare Cost and Utilization Project (HCUP). June 2016. Agency for Healthcare Research and Quality, Rockville, MD. hcup-us.ahrq.gov/reports/statbriefs/sb206-HIV-Hospital-Stays-Trends.jsp. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| If you are experiencing issues related to Section 508 accessibility of information on this website, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 6/20/16 |