STATISTICAL BRIEF #230 |
October 2017
Kathryn R. Fingar, Ph.D., M.P.H., Marguerite L. Barrett, M.S., and H. Joanna Jiang, Ph.D. Introduction There have been increasing efforts among healthcare policy makers, payers, and providers to measure and reduce hospital readmissions. Various time frames are used for identifying readmissions: 48 hours,1 7 days,2 15 days,3,4 and 30 days after discharge of an initial stay.5,6,7 The likelihood of readmission and associated contributing factors vary by the length of postdischarge time.8,9 Thus, it is important to understand how readmission rates and the conditions associated with the highest readmission rates vary by different postdischarge time frames. This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data on rates of all-cause 7-day readmissions compared with all-cause 30-day readmissions in 2014. For diagnoses with the highest 7-day readmission rates, the percentage of 30-day readmissions that occurred within 7 days is also presented. Finally, 7-day and 30-day readmission rates are reported by expected payer. Readmissions include stays for all causes, including planned and unplanned stays. Readmission rates reported by diagnoses reflect the principal diagnosis at the index (i.e., initial) inpatient stay, grouped into broad clinical categories. Condition-specific readmission rates for index stays related to nonspecific clinical categories (e.g., other respiratory diseases), cancer, and pregnancy are not reported. However, these stays contribute to the total readmission rate. All differences between estimates noted in the text are greater than 10 percent. Findings Diagnoses with the highest readmission rates, 2014 Table 1 presents all-cause 7-day readmission rates following index stays overall and for the top 20 principal diagnoses at the index stay. The top 20 diagnoses with the highest 30-day readmission rates also are shown for comparison. The diagnoses are sorted by the 7-day readmission rate. |
|
| Table 1. Top 20 principal diagnoses with the highest 7-day and 30-day readmission rates, 2014 | |||||
| Principal diagnosis at the index stay | Index stays, N | 7-day readmissions | 30-day readmissions | ||
|---|---|---|---|---|---|
| Rank | Ratea | Rank | Ratea | ||
| Total inpatient stays | 27,698,101 | - | 5.0 | - | 13.9 |
| Schizophrenia and other psychotic disorders | 374,097 | 1 | 9.0 | 2 | 22.9 |
| Alcohol-related disorders | 340,076 | 2 | 7.5 | 4 | 21.5 |
| Congestive heart failure; nonhypertensive | 795,709 | 3 | 7.4 | 1 | 23.2 |
| Heart valve disorders | 117,788 | 4 | 7.3 | 14 | 18.4 |
| Hypertension with complications, secondary hypertension | 223,396 | 5 | 7.2 | 6 | 20.9 |
| Respiratory failure; insufficiency; arrest (adult) | 311,005 | 6 | 7.2 | 3 | 21.6 |
| Aspiration pneumonitis; food/vomitus | 128,019 | 7 | 7.1 | 11 | 19.5 |
| Acute and unspecified renal failure | 436,833 | 8 | 7.0 | 8 | 20.1 |
| Diabetes mellitus with complications | 487,947 | 9 | 6.9 | 7 | 20.5 |
| Complication of device; implant or graft | 572,761 | 10 | 6.7 | 10 | 19.7 |
| Septicemia | 1,202,893 | 11 | 6.7 | 13 | 18.5 |
| Deficiency and other anemia | 171,160 | 12 | 6.6 | 5 | 21.2 |
| Intestinal obstruction without hernia | 313,596 | 13 | 6.6 | 25 | 15.2 |
| Fluid and electrolyte disorders | 338,954 | 14 | 6.5 | 12 | 18.8 |
| Abdominal pain | 113,331 | 15 | 6.5 | 18 | 17.2 |
| Complications of surgical procedures or medical care | 417,261 | 16 | 6.5 | 15 | 17.9 |
| Gastrointestinal hemorrhage | 331,739 | 17 | 6.5 | 20 | 16.9 |
| Pancreatic disorders (not diabetes) | 276,534 | 18 | 6.2 | 17 | 17.2 |
| Chronic obstructive pulmonary disease and bronchiectasis | 521,955 | 19 | 6.1 | 9 | 20.1 |
| Acute myocardial infarction | 480,338 | 20 | 6.1 | 29 | 14.2 |
| Intestinal infection | 195,644 | 24 | 5.7 | 16 | 17.5 |
| Peripheral and visceral atherosclerosis | 127,624 | 22 | 5.8 | 19 | 16.9 |
| Notes: Diagnoses are grouped using the Clinical Classification Software (CCS). Only CCS with at least 100,000 index stays are shown; "other" CCS that group a nonspecific set of diagnoses, as well as diagnoses related to cancer and pregnancy, are excluded. Highlighting indicates diagnoses that were not ranked in the top 20 for either 7-day or 30-day readmissions. a Rate per 100 index inpatient stays Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Readmissions Database (NRD), 2014 | |||||
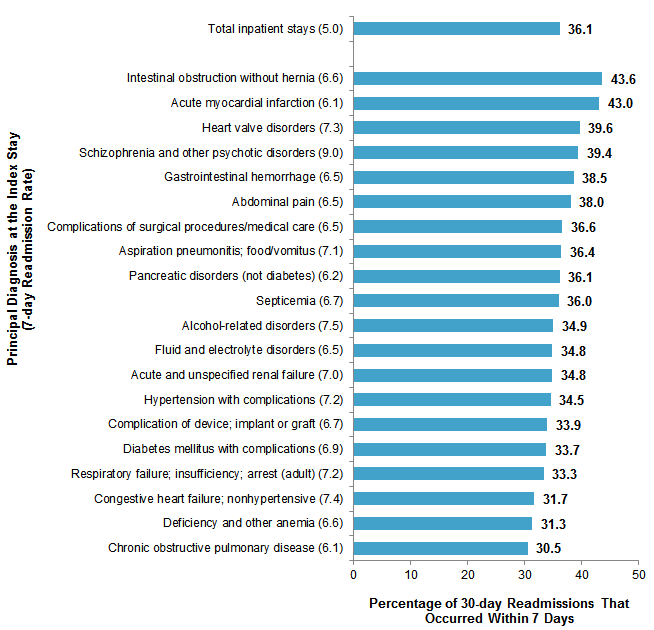
Figure 1 displays the percentage of 30-day readmissions that occurred within 7 days following discharge, overall and for the top 20 principal diagnoses with the highest 7-day readmission rates. The 7-day readmission rate is listed on the y-axis for reference. |
|
Figure 1. The percentage of 30-day readmissions that occurred within 7 days, overall and for the top 20 diagnoses with the highest 7-day readmission rates, 2014
Notes: Readmission rates are per 100 index inpatient stays. The principal diagnosis is grouped using the Clinical Classification Software (CCS). Only CCS with at least 100,000 index stays are shown; "other" CCS that group a nonspecific set of diagnoses, as well as diagnoses related to cancer and pregnancy, are excluded. Bar chart shows percentage of 30-day readmissions that occurred within 7 days by principal diagnosis with highest 7-day readmission rate in 2014. Total inpatient stays (7-day readmission rate=5.0): 36.1%. Intestinal obstruction without hernia (7-day readmission rate=6.6): 43.6%. Acute myocardial infarction (7-day readmission rate=6.1): 43.0%. Heart valve disorders (7-day readmission rate=7.3): 39.6%. Schizophrenia and other psychotic disorders (7-day readmission rate=9.0): 39.4%. Gastrointestinal hemorrhage (7-day readmission rate=6.5): 38.5%. Abdominal pain (7-day readmission rate=6.5): 38.0%. Complications of surgical procedures/medical care (7-day readmission rate=6.5): 36.6%. Aspiration pneumonitis; food/vomitus (7-day readmission rate=7.1): 36.4%. Pancreatic disorders (not diabetes) (7-day readmission rate=6.2): 36.1%. Septicemia (7-day readmission rate=6.7): 36.0%. Alcohol-related disorders (7-day readmission rate=7.5): 34.9%. Fluid and electrolyte disorders (7-day readmission rate=6.5): 34.8%. Acute and unspecified renal failure (7-day readmission rate=7.0): 34.8%. Hypertension with complications (7-day readmission rate=7.2): 34.5%. Complication of device; implant or graft (7-day readmission rate=6.7): 33.9%. Diabetes mellitus with complications (7-day readmission rate=6.9): 33.7%. Respiratory failure; insufficiency; arrest (adult) (7-day readmission rate=7.2): 33.3. Congestive heart failure; nonhypertensive (7-day readmission rate=7.4): 31.7%. Deficiency and other anemia (7-day readmission rate=6.6): 31.3%. Chronic obstructive pulmonary disease (7-day readmission rate=6.1): 30.5%.
|
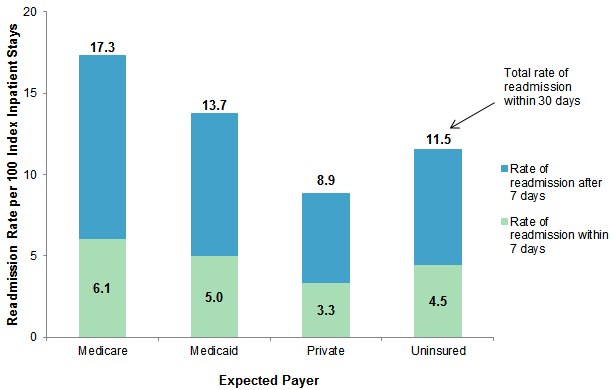
Figure 2 displays all-cause 7-day and 30-day readmission rates following index stays by expected payer. |
|
Figure 2. All-cause 7-day and 30-day readmission rates, by expected payer, 2014
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Readmissions Database (NRD), 2014 Bar chart that shows readmission rate per 100 index inpatient stays by expected payer in 2014. Medicare: total readmission rate within 30 days: 17.3; readmission rate within 7 days: 6.1. Medicaid: total readmission rate within 30 days: 13.7; readmission rate within 7 days: 5.0. Private: total readmission rate within 30 days: 8.9; readmission rate within 7 days: 3.3. Uninsured: total readmission rate within 30 days: 11.5; readmission rate within 7 days: 4.5.
|
|
| Table 2. Top five principal diagnoses with the highest 7-day and 30-day readmission rates, by expected payer, 2014 | |||||
| Principal diagnosis | Index stays, N | 7-day readmissions | 30-day readmissions | ||
|---|---|---|---|---|---|
| Rank | Ratea | Rank | Ratea | ||
| Medicare | |||||
| Schizophrenia and other psychotic disorders | 150,743 | 1 | 9.3 | 3 | 23.9 |
| Pleurisy; pneumothorax; pulmonary collapse | 50,119 | 2 | 8.9 | 1 | 24.5 |
| Alcohol-related disorders | 67,838 | 3 | 8.3 | 2 | 24.4 |
| Heart valve disorders | 85,682 | 4 | 7.9 | 14 | 19.9 |
| Hypertension with complications, secondary hypertension | 141,206 | 5 | 7.7 | 8 | 22.6 |
| Deficiency and other anemia | 103,430 | 13 | 7.1 | 4 | 23.3 |
| Congestive heart failure; nonhypertensive | 613,829 | 9 | 7.4 | 5 | 23.3 |
| Medicaid | |||||
| Schizophrenia and other psychotic disorders | 151,794 | 1 | 9.9 | 6 | 24.9 |
| Sickle cell anemia | 50,187 | 2 | 9.8 | 1 | 34.4 |
| Alcohol-related disorders | 123,583 | 3 | 9.3 | 3 | 26.1 |
| Congestive heart failure; nonhypertensive | 78,938 | 4 | 9.0 | 2 | 28.5 |
| Hypertension with complications, secondary hypertension | 33,068 | 5 | 8.9 | 4 | 25.0 |
| Complication of device; implant or graft | 71,974 | 6 | 8.5 | 5 | 25.0 |
| Private | |||||
| Acute and unspecified renal failure | 54,314 | 1 | 6.4 | 3 | 17.2 |
| Regional enteritis and ulcerative colitis | 42,829 | 2 | 6.4 | 4 | 16.2 |
| Schizophrenia and other psychotic disorders | 35,493 | 3 | 6.2 | 5 | 15.8 |
| Congestive heart failure; nonhypertensive | 67,683 | 4 | 6.0 | 1 | 18.7 |
| Deficiency and other anemia | 29,565 | 5 | 6.0 | 2 | 17.6 |
| Uninsured | |||||
| Schizophrenia and other psychotic disorders | 23,574 | 1 | 7.4 | 4 | 17.3 |
| Abdominal pain | 9,104 | 2 | 6.8 | 8 | 16.2 |
| Alcohol-related disorders | 56,753 | 3 | 6.5 | 1 | 18.2 |
| Mood disorders | 82,318 | 4 | 6.5 | 11 | 15.3 |
| Complications of surgical procedures or medical care | 11,261 | 5 | 6.3 | 7 | 16.8 |
| Regional enteritis and ulcerative colitis | 6,630 | —b | —b | 2 | 18.1 |
| Complication of device; implant or graft | 8,777 | 7 | 6.1 | 3 | 18.1 |
| Congestive heart failure; nonhypertensive | 21,986 | 12 | 5.2 | 5 | 17.0 |
| a Rate per 100 index inpatient stays b Data are suppressed because cell contains fewer than 11 readmissions. Note: Diagnoses are grouped using the Clinical Classification Software (CCS). Only CCS with at least 50,000 Medicare index stays, 20,000 Medicaid index stays, 25,000 privately insured index stays, and 5,000 uninsured index stays are shown. "Other" CCS that group a nonspecific set of diagnoses, as well as diagnoses related to cancer and pregnancy, are excluded. Highlighting indicates diagnoses that were not ranked in the top five for either 7-day or 30-day readmissions. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Readmissions Database (NRD), 2014 | |||||
|
|
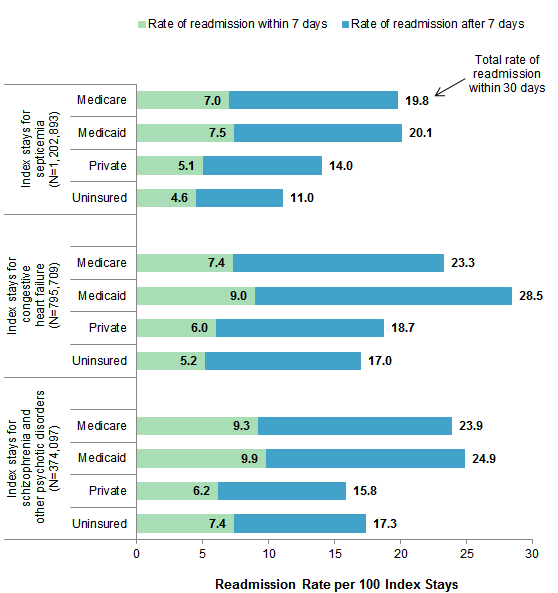
Figure 3. All-cause 7-day and 30-day readmission rates following index stays for three select conditions, by expected payer, 2014
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Readmissions Database (NRD), 2014 Bar chart that shows 7- and 30-day readmission rates following index stays for septicemia (N=1,202,893), congestive heart failure (N=795,709), and schizophrenia and other psychotic disorders (N=374,097), by expected payer in 2014. Septicemia: Medicare: readmission rate within 7 days: 7.0; total readmission rate within 30 days: 19.8. Medicaid: readmission rate within 7 days: 7.5; total readmission rate within 30 days: 20.1. Private: readmission rate within 7 days: 5.1; total readmission rate within 30 days: 14.0. Uninsured: readmission rate within 7 days: 4.6; total readmission rate within 30 days: 11.0. Congestive heart failure: Medicare: readmission rate within 7 days: 7.4; total readmission rate within 30 days: 23.3. Medicaid: readmission rate within 7 days: 9.0; total readmission rate within 30 days: 28.5. Private: readmission rate within 7 days: 6.0; total readmission rate within 30 days: 18.7. Uninsured: readmission rate within 7 days: 5.2; total readmission rate within 30 days: 17.0. Schizophrenia and other psychotic disorders: Medicare: readmission rate within 7 days: 9.3; total readmission rate within 30 days: 23.9. Medicaid: readmission rate within 7 days: 9.9; total readmission rate within 30 days: 24.9. Private: readmission rate within 7 days: 6.2; total readmission rate within 30 days: 15.8. Uninsured: readmission rate within 7 days: 7.4; total readmission rate within 30 days: 17.3.
|
|
| Table 3. All-cause 7-day readmissions as a percentage of 30-day readmissions following index stays for three select conditions, by expected payer, 2014 | ||||||
| Expected payer | Septicemia | Congestive heart failure | Schizophrenia and other psychotic disorders | |||
|---|---|---|---|---|---|---|
| Number of 30-day readmissions | 30-day readmissions within 7 days, % | Number of 30-day readmissions | 30-day readmissions within 7 days, % | Number of 30-day readmissions | 30-day readmissions within 7 days, % | |
| Medicare | 155,652 | 35.5 | 142,967 | 31.7 | 36,015 | 38.8 |
| Medicaid | 32,408 | 37.1 | 22,464 | 31.8 | 37,762 | 39.7 |
| Private | 25,848 | 36.3 | 12,685 | 32.3 | 5,625 | 39.2 |
| Uninsured | 5,102 | 41.4 | 3,738 | 30.5 | 4,087 | 42.7 |
| Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), Nationwide Readmissions Database (NRD), 2014 | ||||||
HCUP Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) 2014 Nationwide Readmissions Database (NRD). Definitions Diagnoses and Clinical Classifications Software (CCS) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.10 This clinical grouper makes it easier to quickly understand patterns of diagnoses use. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. Readmissions The 30-day readmission rate is defined as the number of admissions for each condition for which there was at least one subsequent hospital admission within 7 or 30 days, divided by the total number of admissions from January through November of the same year. That is, when patients are discharged from the hospital, they are followed for 7 or 30 days in the data. If any readmission to the same or different hospital occurs during the specified time period, the admission is counted as having a readmission. No more than one readmission is counted within the 7- or 30-day period, because the outcome measure assessed is "percentage of admissions that are readmitted." If a patient was transferred to a different hospital on the same day or was transferred within the same hospital, the two events were combined as a single stay and the second event was not counted as a readmission; that is, transfers were not considered a readmission. Every qualifying inpatient stay is counted as a separate initial (starting point) admission, called an index stay. Thus, a single patient can be counted multiple times during the course of the January through November observation period. In addition, index stays do not require a prior "clean period" with no hospitalizations; that is, a hospital stay may be a readmission for a prior stay and the initial admission for a subsequent readmission. Admissions were disqualified from the analysis as index stays if they could not be followed for 7 or 30 days for one of the following reasons: (1) the patient died in the hospital, (2) information on length of stay was missing, or (3) the patient was discharged in December. Types of hospitals included in the HCUP Nationwide Readmissions Database The Nationwide Readmissions Database (NRD) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NRD includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, long-term acute care, psychiatric, and alcoholism and chemical dependency hospitals. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NRD. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For this Statistical Brief, a hierarchy was used to assign the payer category based on the primary and secondary expected payer:11
About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NRD The HCUP Nationwide Readmissions Database (NRD) is a calendar-year, discharge-level database constructed from the HCUP State Inpatient Databases (SID) with verified patient linkage numbers that can be used to track a person across hospitals within a State. The 2010-2014 NRD is available for purchase through the HCUP Central Distributor. The NRD is designed to support various types of analyses of national readmission rates. The database includes discharges for patients with and without repeat hospital visits in a year and those who have died in the hospital. Repeat stays may or may not be related. The criteria to determine the relationship between hospital admissions are left to the analyst using the NRD. The NRD was constructed as a sample of convenience consisting of 100 percent of the eligible discharges. Discharge weights for national estimates are developed using the target universe of community hospitals (excluding rehabilitation and long-term acute care hospitals) in the United States. Over time, the sampling frame for the NRD will change; thus, the number of States contributing to the NRD will vary from year to year. The NRD is intended for national estimates only; no regional, State-, or hospital-specific estimates can be produced. For More Information For other information on readmissions and revisits, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_readmission.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the Nationwide Readmissions Database (NRD), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the Nationwide Readmissions Database (NRD). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated December 2016. www.hcup-us.ahrq.gov/nrdoverview.jsp. Accessed January 31, 2017. Suggested Citation Fingar KR (IBM Watson Health), Barrett ML (M.L. Barrett, Inc.), Jiang HJ (AHRQ). A Comparison of All-Cause 7-Day and 30-Day Readmissions, 2014. HCUP Statistical Brief #230. October 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb230-7-Day-Versus-30-Day-Readmissions.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Sharon B. Arnold, Ph.D., Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on October 31, 2017. 1 Colorado Medical Association. Inpatient/Outpatient Billing Manual. February 2014. www.colorado.gov/pacific/sites/default/files/IP%20and%20OP%20Hospital%20Billing%20Manual%20(February%202014).pdf. 2 Chin DL, Bang H, Manickam RN, Romano PS. Rethinking Thirty-Day Hospital Readmissions: Shorter Intervals Might Be Better Indicators of Quality of Care. Health Affairs (Millwood). 2016;35(10):1867-75. 3 Michigan Department of Health and Human Services. Medicaid Provider Manual. July 2017. www.mdch.state.mi.us/dch-medicaid/manuals/MedicaidProviderManual.pdf. 4 Texas External Quality Review Organization. Potentially Preventable Readmissions in Texas Medicaid and CHIP Programs. December 2014. hhs.texas.gov/sites/default/files/documents/about-hhs/process-improvement/medicaid-chip-qei/PPR-Statewide-Report-FY2013.pdf. 5 Ibid. 6 Centers for Medicare & Medicaid Services. Hospital Readmissions Reduction Program (HRRP). April 2016. www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed June 6, 2017. 7 Washington State Health Care Authority. Potentially Preventable Readmissions (PPR) Policy. Frequently Asked Questions (FAQ) - CY 2016. February 2016. www.wsha.org/wp-content/uploads/WA-PPR-FAQ-Final.pdf. 8 Chin et al., 2016. Op. cit. 9 Herrin J, St Andre J, Kenward K, Joshi MS, Audet AM, Hines SC. Community factors and hospital readmission rates. Health Services Research. 2015;50(1):20-39. 10 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated October 2016. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed January 31, 2017. 11 The 2013 NRD available for purchase through the HCUP Central Distributor includes the data element for the primary expected payer but not the data element for the secondary expected payer. |
| Internet Citation: Statistical Brief #230. Healthcare Cost and Utilization Project (HCUP). October 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb230-7-Day-Versus-30-Day-Readmissions.jsp?utm_source=ahrq&utm_medium=en1&utm_term. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 10/25/17 |