STATISTICAL BRIEF #232 |
December 2017
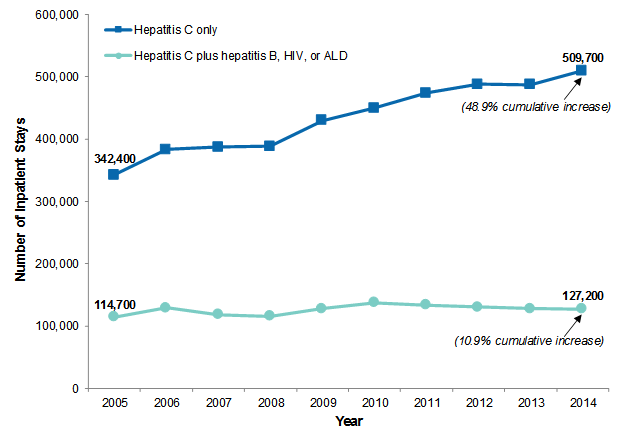
Quyen Ngo-Metzger, M.D., M.P.H., Iris Mabry-Hernandez, M.D., Kevin C. Heslin, Ph.D., Audrey J. Weiss, Ph.D., Amanda Mummert, Ph.D., and Arlene S. Bierman, M.D., M.S. Introduction Hepatitis C virus is the most common chronic blood-borne pathogen in the United States.1 The number of people in the United States with hepatitis C is estimated at 4.6 million, of whom an estimated 3.2 million are chronically infected.2,3,4 Based on data from 1999 to 2008, about three-fourths of individuals in the United States now living with hepatitis C were born between 1945 and 1965 (baby boomers), with a prevalence of 3.3 percent.5 The most important risk factor for hepatitis C is current or past injection drug use.6 Acute hepatitis C cases nearly tripled from 2010 through 2015, likely the result of increasing injection drug use due to the growing opioid epidemic.7,8 People with hepatitis C can have a mild, short-term illness. However, 75-85 percent of those who become infected with hepatitis C develop a chronic infection that can result in cirrhosis, liver failure, hepatocellular carcinoma (liver cancer), and death.9 Factors associated with the progression of liver disease in people with chronic hepatitis C include coinfection with hepatitis B virus, coinfection with human immunodeficiency virus (HIV), and high levels of alcohol intake.10 Chronic hepatitis C virus is the most common indication for liver transplants among U.S. adults.11 Mortality rates from hepatitis C have been increasing. From 1999 to 2007, the average annual age-adjusted mortality rate involving hepatitis C increased by 0.18 deaths per 100,000 population.12 The rate of hospitalizations associated with hepatitis C also has increased significantly, from 4.8 per 100,000 population in 2004-2005 to 13.8 per 100,000 population in 2010-2011 (a 190-percent increase).13 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data for adults aged 18 years and older on hepatitis C-related inpatient stays, including those among patients with and without key co-occurring diagnoses: hepatitis B, HIV, and alcoholic liver disease (ALD). Trends in the number and population rate of hepatitis C-related inpatient stays from 2005 through 2014 are provided. Characteristics of hepatitis C-related inpatient stays in 2014 are presented by patient age group and by presence or absence of the key codiagnoses. Because hepatitis C is so prevalent among baby boomers, characteristics and codiagnoses of hepatitis C-related stays are further detailed specifically for this age group. Finally, the rate of hepatitis C-related inpatient stays in 2014 is depicted by U.S. census division for each patient age group. Differences in estimates of 10 percent or greater are noted in the text. Findings Trends in hepatitis C-related inpatient stays, 2005-2014 Figure 1 presents trends in the number of inpatient stays involving hepatitis C—with and without hepatitis B, human immunodeficiency virus (HIV), or alcoholic liver disease (ALD)—among adults aged 18 years and older from 2005 through 2014. |
|
|
Figure 1. Number of inpatient stays involving hepatitis C among adults aged 18+ years, 2005-2014
Abbreviations: ALD, alcoholic liver disease; HIV, human immunodeficiency virus Line graph that shows the number of inpatient stays involving hepatitis C only or hepatitis C plus hepatitis B, human immunodeficiency virus, or alcoholic liver disease among adults aged 18+ years from 2005 to 2014. Hepatitis C only—2005: 342,400; 2006: 382,900; 2007: 386,800; 2008: 388,400; 2009: 429,600; 2010: 449,300; 2011, 473,900; 2012, 487,800; 2013, 487,100; 2014: 509,700; cumulative increase: 48.9%. Hepatitis C plus hepatitis B, human immunodeficiency virus, or alcoholic liver disease—2005: 114,700; 2006: 128,900; 2007: 118,000; 2008: 115,600; 2009: 128,100; 2010: 137,200; 2011, 133,700; 2012, 130,100; 2013, 128,200; 2014: 127,200; cumulative increase: 10.9%.
|
|
|
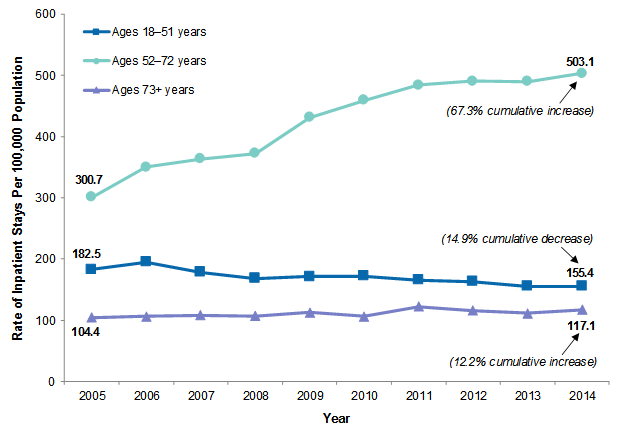
Figure 2. Rate of inpatient stays involving hepatitis C by patient age group, 2005-2014
Note: All stays involving hepatitis C are included—those stays with and without hepatitis B, human immunodeficiency virus (HIV), and alcoholic liver disease. Line graph showing the rate of inpatient stays involving hepatitis C per 100,000 population by age from 2005 to 2014. Ages 18-51 years—2005: 182.5; 2006: 195.1; 2007: 178.3; 2008: 168.0; 2009: 171.4; 2010: 172.2; 2011: 165.4; 2012: 163.1; 2013: 155.6; 2014: 155.4; cumulative decrease: 14.9%. Ages 52-72 years—2005: 300.7; 2006: 349.8; 2007: 363.2; 2008: 372.2; 2009: 430.7; 2010: 458.8; 2011: 484.0; 2012: 490.2; 2013: 489.4; 2014: 503.1; cumulative increase: 67.3%. Ages 73+ years—2005: 104.4; 2006: 106.0; 2007: 108.1; 2008: 106.9; 2009: 112.9; 2010: 106.2; 2011: 122.0; 2012: 115.5; 2013: 111.2; 2014: 117.1; cumulative increase: 12.2%.
|
Table 1 presents utilization and patient characteristics for all inpatient stays involving hepatitis C by patient age group in 2014. Characteristics of adult inpatients stays that do not involve hepatitis C are provided for comparison. |
| Table 1. Characteristics of inpatient stays involving hepatitis C by patient age group, 2014 | |||||
| Characteristic | Hepatitis C | No hepatitis C | |||
|---|---|---|---|---|---|
| 18-51 years | 52-72 years | 73+ years | All adults 18+ years | All adults 18+ years | |
| Number of stays | 225,900 | 383,200 | 27,800 | 636,900 | 29,115,100 |
| Rate of stays (per 100,000 population) | 155.4 | 503.1 | 117.1 | 259.7 | 11,870.5 |
| Utilization characteristics | |||||
| Cost per stay, mean $ | 11,000 | 14,600 | 14,500 | 13,300 | 11,600 |
| Length of stay, mean days | 5.5 | 6.0 | 6.1 | 5.8 | 4.7 |
| Died during hospital stay, % | 1.5 | 3.5 | 5.3 | 2.9 | 2.2 |
| Patient characteristics | |||||
| Sex, % | |||||
| Male | 54.7 | 66.5 | 47.9 | 61.5 | 40.7 |
| Female | 45.3 | 33.5 | 52.1 | 38.5 | 59.3 |
| Race/ethnicity, % | |||||
| White | 67.1 | 54.5 | 52.7 | 58.9 | 65.0 |
| Black | 11.4 | 26.5 | 21.4 | 20.9 | 13.9 |
| Hispanic | 12.1 | 10.9 | 12.5 | 11.4 | 10.1 |
| Other | 4.6 | 4.5 | 10.1 | 4.7 | 5.9 |
| Expected primary payer, % | |||||
| Medicare | 17.6 | 41.3 | 90.0 | 35.0 | 46.6 |
| Medicaid | 52.9 | 32.0 | 2.8 | 38.1 | 17.4 |
| Private insurance | 12.3 | 17.1 | 5.2 | 14.9 | 28.4 |
| Uninsured | 13.0 | 5.4 | 0.5 | 7.9 | 4.7 |
| Other | 3.8 | 3.9 | 1.4 | 3.8 | 2.8 |
| Community-level income, % | |||||
| Low income (<$40,000) | 40.9 | 40.1 | 30.4 | 40.0 | 28.8 |
| Not low income ($40,000+) | 59.1 | 59.9 | 69.6 | 60.0 | 71.2 |
| Location, % | |||||
| Large central metropolitan | 31.4 | 40.1 | 47.0 | 37.3 | 29.5 |
| Large fringe metropolitan | 20.6 | 19.8 | 22.4 | 20.2 | 24.0 |
| Medium metropolitan | 20.9 | 19.5 | 15.7 | 19.8 | 20.1 |
| Small metropolitan | 8.6 | 7.6 | 6.3 | 7.9 | 9.3 |
| Micropolitan | 9.1 | 6.6 | 4.7 | 7.4 | 9.4 |
| Noncore (rural) | 6.9 | 4.3 | 3.4 | 5.2 | 7.2 |
| Notes: All stays involving hepatitis C are included—those stays with and without hepatitis B, human immunodeficiency virus (HIV), and alcoholic liver disease. Number of stays and cost per stay are rounded to the nearest 100. Location is missing for approximately 2.2 percent of stays with hepatitis C and 0.5 percent of stays without hepatitis C. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | |||||
|
| Table 2. Co-occurring diagnoses, procedures, and comorbidities associated with inpatient stays involving hepatitis C by patient age group, 2014 | |||||
| Diagnosis, procedure, or comorbidity | Hepatitis C | No hepatitis C | |||
|---|---|---|---|---|---|
| 18-51 years | 52-72 years | 73+ years | All adults 18+ years | All adults 18+ years | |
| Diagnosis, % | |||||
| Hepatitis C (principal diagnosis) | 3.7 | 6.3 | 5.0 | 5.3 | - |
| Hepatitis B | 3.4 | 3.2 | 2.4 | 3.3 | 0.2 |
| HIV | 7.1 | 6.1 | 1.3 | 6.2 | 0.6 |
| Alcoholic liver disease (ALD) | 9.1 | 13.6 | 3.3 | 11.5 | 1.1 |
| Liver cancer | 1.0 | 6.2 | 8.3 | 4.5 | 1.1 |
| Cirrhosis of the liver | 9.7 | 23.8 | 29.6 | 19.1 | 0.8 |
| Ascites | 7.2 | 14.7 | 12.7 | 12.0 | 1.2 |
| Upper GI bleeding | 4.5 | 7.1 | 7.1 | 6.2 | 2.3 |
| Any mental disorder | 78.4 | 69.7 | 42.4 | 71.6 | 44.3 |
| Any nonalcohol SUD | 53.5 | 24.9 | 4.8 | 34.2 | 5.7 |
| Any alcohol-related diagnosis (not ALD) | 26.8 | 26.9 | 6.3 | 26.0 | 5.7 |
| Procedure, % | |||||
| Abdominal paracentesis | 4.1 | 8.8 | 6.7 | 7.0 | 0.9 |
| Upper GI endoscopy | 4.8 | 7.3 | 7.5 | 6.4 | 3.6 |
| Comorbidity, % | |||||
| Hypertension | 30.1 | 58.3 | 71.9 | 48.9 | 49.8 |
| Fluid and electrolyte disorders | 26.8 | 37.2 | 40.2 | 33.7 | 24.6 |
| Drug abuse | 44.8 | 22.1 | 4.2 | 29.4 | 4.6 |
| Chronic pulmonary disease | 19.5 | 29.2 | 26.4 | 25.6 | 18.7 |
| Deficiency anemias | 17.3 | 25.7 | 31.7 | 22.9 | 17.5 |
| Alcohol abuse | 20.5 | 23.3 | 5.8 | 21.5 | 4.6 |
| Diabetes, uncomplicated | 11.0 | 23.4 | 28.6 | 19.2 | 18.9 |
| Coagulopathy | 13.3 | 22.0 | 22.7 | 19.0 | 4.9 |
| Depression | 15.8 | 16.0 | 10.8 | 15.7 | 11.3 |
| Renal failure | 6.9 | 18.5 | 32.1 | 15.0 | 12.6 |
| Psychoses | 17.2 | 11.8 | 4.5 | 13.4 | 4.8 |
| Other neurological disorders | 9.7 | 9.1 | 10.1 | 9.4 | 7.6 |
| Obesity | 8.4 | 10.0 | 6.4 | 9.3 | 13.4 |
| Congestive heart failure | 3.7 | 10.5 | 20.2 | 8.5 | 8.9 |
| Hypothyroidism | 5.1 | 8.7 | 19.2 | 7.9 | 11.9 |
| Weight loss | 5.1 | 9.2 | 11.2 | 7.8 | 4.9 |
| Diabetes with chronic complications | 3.6 | 7.8 | 8.2 | 6.3 | 5.1 |
| Peripheral vascular disorders | 1.7 | 6.5 | 11.5 | 5.0 | 6.1 |
| Abbreviations: GI, gastrointestinal; HIV, human immunodeficiency virus; SUD, substance use disorder Note: All stays involving hepatitis C are included—those stays with and without hepatitis B, HIV, and ALD. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | |||||
Table 3 presents utilization and patient characteristics among baby boomers for hepatitis C-related inpatient stays with and without hepatitis B, HIV, or ALD. Characteristics of inpatient stays that do not involve hepatitis C among baby boomers are provided for comparison. |
| Table 3. Characteristics of inpatient stays involving hepatitis C among baby boomers, 2014 | |||
| Characteristic | Ages 52-72 years (baby boomers) | ||
|---|---|---|---|
| Hepatitis C without hepatitis B, HIV, or ALD | Hepatitis C plus hepatitis B, HIV, or ALD | No hepatitis C | |
| Number of stays | 300,000 | 83,300 | 10,282,100 |
| Percentage of all baby boomer stays | 2.8 | 0.8 | 96.4 |
| Rate of stays (per 100,000 population) | 393.8 | 109.3 | 13,498.2 |
| Utilization characteristics | |||
| Cost per stay, mean $ | 14,500 | 15,000 | 14,100 |
| Length of stay, mean days | 5.9 | 6.4 | 5.1 |
| Died during hospital stay, % | 3.1 | 5.1 | 2.2 |
| Patient characteristics | |||
| Sex, % | |||
| Male | 64.6 | 73.6 | 50.2 |
| Female | 35.4 | 26.4 | 49.8 |
| Race/ethnicity, % | |||
| White | 55.7 | 50.1 | 68.2 |
| Black | 26.1 | 27.9 | 14.0 |
| Hispanic | 10.1 | 13.6 | 7.9 |
| Other | 4.4 | 4.7 | 4.9 |
| Expected primary payer, % | |||
| Medicare | 42.6 | 36.4 | 50.2 |
| Medicaid | 29.8 | 39.7 | 11.6 |
| Private insurance | 18.0 | 13.9 | 31.0 |
| Uninsured | 5.2 | 6.4 | 3.9 |
| Other | 4.1 | 3.5 | 3.1 |
| Community-level income, % | |||
| Low income (<$40,000) | 40.0 | 40.4 | 29.6 |
| Not low income ($40,000+) | 60.0 | 59.6 | 70.4 |
| Location, % | |||
| Large central metropolitan | 40.2 | 39.7 | 28.1 |
| Large fringe metropolitan | 20.5 | 17.4 | 23.8 |
| Medium metropolitan | 19.7 | 18.7 | 20.2 |
| Small metropolitan | 7.8 | 7.2 | 9.6 |
| Micropolitan | 6.7 | 6.1 | 10.0 |
| Noncore (rural) | 4.4 | 3.8 | 7.9 |
| Abbreviations: ALD, alcoholic liver disease; HIV, human immunodeficiency virus Notes: Number of stays and cost per stay are rounded to the nearest 100. Location is missing for approximately 0.7 percent of stays with hepatitis C only, 7.1 percent of stays with hepatitis C-plus, and 0.4 percent of stays without hepatitis C. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | |||
|
| Table 4. Co-occurring diagnoses, procedures, and comorbidities associated with inpatient stays involving hepatitis C among baby boomers, 2014 | |||
| Diagnosis, procedure, or comorbidity | Ages 52-72 years (baby boomers) | ||
|---|---|---|---|
| Hepatitis C without hepatitis B, HIV, or ALD | Hepatitis C plus hepatitis B, HIV, or ALD | No hepatitis C | |
| Diagnosis, % | |||
| Hepatitis C (principal diagnosis) | 5.4 | 9.7 | - |
| Hepatitis B | - | 14.8 | 0.2 |
| HIV | - | 28.0 | 0.6 |
| Alcoholic liver disease (ALD) | - | 62.4 | 1.6 |
| Liver cancer | 5.8 | 7.7 | 1.7 |
| Cirrhosis of the liver | 27.6 | 10.2 | 1.3 |
| Ascites | 11.1 | 27.7 | 1.8 |
| Upper GI bleeding | 5.5 | 13.1 | 2.6 |
| Any mental disorder | 69.8 | 69.5 | 53.4 |
| Any nonalcohol SUD | 24.3 | 27.2 | 4.5 |
| Any alcohol-related diagnosis (not ALD) | 18.0 | 59.0 | 7.3 |
| Procedure, % | |||
| Abdominal paracentesis | 6.4 | 17.6 | 1.3 |
| Upper GI endoscopy | 6.2 | 11.1 | 4.1 |
| Comorbidity, % | |||
| Hypertension | 60.4 | 50.8 | 63.3 |
| Fluid and electrolyte disorders | 35.4 | 44.0 | 27.8 |
| Drug abuse | 21.4 | 24.5 | 3.6 |
| Chronic pulmonary disease | 29.6 | 27.5 | 23.5 |
| Deficiency anemias | 24.6 | 29.6 | 18.2 |
| Alcohol abuse | 14.8 | 53.7 | 6.1 |
| Diabetes, uncomplicated | 24.4 | 19.6 | 25.8 |
| Coagulopathy | 18.6 | 34.3 | 5.6 |
| Depression | 16.3 | 14.9 | 14.1 |
| Renal failure | 18.7 | 17.6 | 13.7 |
| Psychoses | 11.9 | 11.5 | 5.7 |
| Other neurological disorders | 9.2 | 9.0 | 7.7 |
| Obesity | 10.9 | 6.7 | 18.5 |
| Congestive heart failure | 10.9 | 9.0 | 9.4 |
| Hypothyroidism | 9.4 | 6.3 | 12.7 |
| Weight loss | 8.3 | 12.5 | 5.7 |
| Diabetes with chronic complications | 8.5 | 5.1 | 7.4 |
| Peripheral vascular disorders | 7.1 | 4.4 | 7.4 |
| Abbreviations: GI, gastrointestinal; HIV, human immunodeficiency virus; SUD, substance use disorder Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | |||
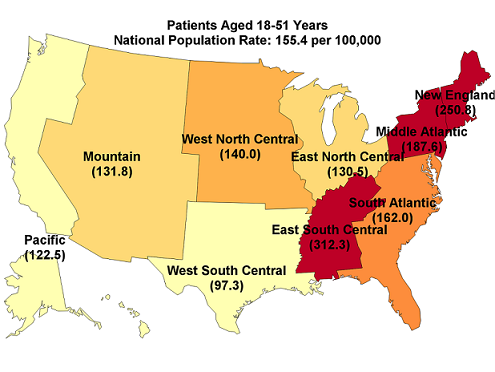
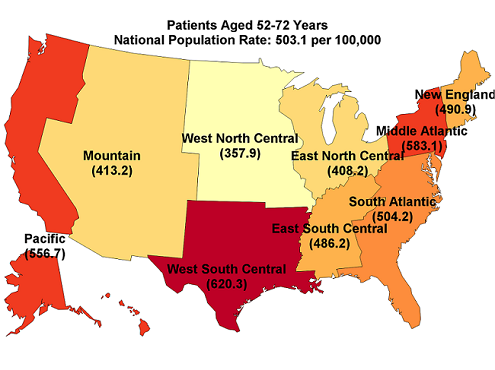
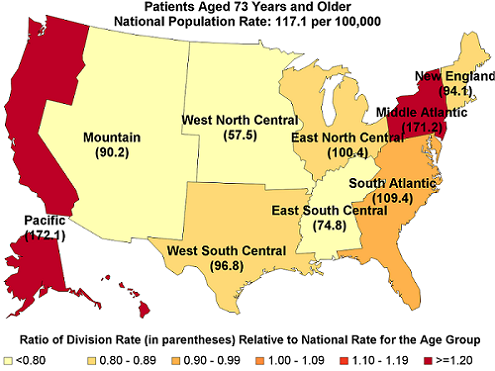
Figure 3 provides the population rate of inpatient stays involving hepatitis C among patients aged 18-51 years, aged 52-72 years, and aged 73+ years by U.S. census division in 2014. The ratio of the census division rate to the national rate for each age group also is provided. |
|
Figure 3. Rate of inpatient stays involving hepatitis C among patients aged 18-51 years, 52-72 years, and 73+ years by census division, and ratio of census division rate to national rate, 2014
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||