STATISTICAL BRIEF #205 |
May 2016
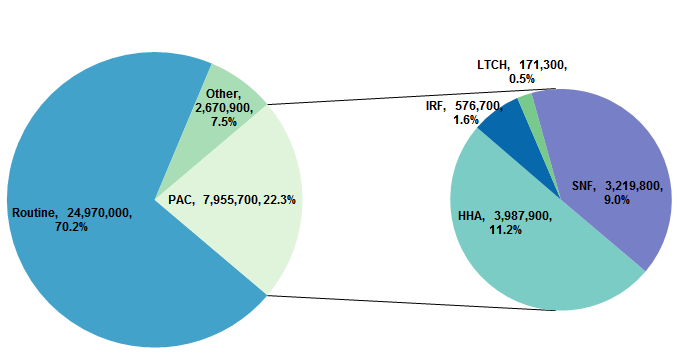
Wen Tian, Ph.D., M.D. Introduction Following hospitalizations for injury or illness, many patients require continued postacute care (PAC) to support recovery, improve functional status, or manage chronic illness. PAC includes a range of medical services such as rehabilitation care, skilled nursing care, and palliative care. In 2014, PAC was provided in 1,177 inpatient rehabilitation facilities (IRFs), 422 long-term care hospitals (LTCHs),15,173 skilled nursing facilities (SNFs), and at home through 12,461 home health agencies (HHAs).1 The four types of PAC settings overlap considerably in the conditions treated. However, each type of setting specializes in a specific array of care and therapies with different staffing, costs, and outcomes.2 About 42 percent of Medicare fee-for-service (FFS) patients were discharged to a PAC setting after hospitalization in 2013.3 Between 2001 and 2013, Medicare spending on PAC, both facility-based and in-home, doubled from $29 billion to $59 billion per year and has grown faster than most other major Medicare spending categories.4 Hospital discharge planning plays a key role in shaping downstream PAC use in terms of the numbers and types of patients discharged to different PAC settings. However, no clear clinical guidance exists to determine the type of PAC setting to which a patient with a specific condition should be discharged. Discharges to PAC often are driven by the availability of specific types of settings and by financial incentives that are not always aligned with clinical needs and may not be cost-effective.5 Current studies on discharges to PAC are based on either Medicare FFS patients using Medicare claims data or small clinic-based cohorts using primary data collection. To date, there are no estimates of discharges to PAC based on a national all-payer dataset that can offer a complete picture including not only Medicare FFS but also other payers. This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data on hospital discharges to PAC settings in 2013 from an all-payer view. Using the 2013 National Inpatient Sample (NIS), this Statistical Brief estimates discharges to PAC for all types of payers and describes these discharges from the perspective of payers, patients, hospitals, conditions/procedures, and geographic regions. Discharges to PAC in this Statistical Brief are defined as those discharges to IRFs, LTCHs, SNFs, or home with HHA services. Discharges to outpatient PAC facilities and inpatient stays in Veterans Health systems are not included because data are not available in the NIS. All differences between estimates noted in the text are statistically significant at the .01 level or better. Findings Discharge disposition and discharges to PAC, 2013 Figure 1 presents the number and percentage of discharges to four types of PAC settings, routine discharges, and other discharges in 2013. |
|
|
Figure 1. Discharge disposition of inpatient stays, 2013
Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility Figure 1 is made up of two pie charts. One pie chart shows the distribution of discharge disposition between routine, postacute care, and other. The second pie chart shows the distribution of discharge disposition for stays discharged to postacute care. Number and percentage of discharges from inpatient stays: routine: 24,970,000, 70.2%; postacute care: 7,955,700, 22.3%; other: 2,670,900, 7.5%. Number and percentage of discharges to postacute care: home health agency: 3,987,900, 11.2%; skilled nursing facility: 3,219,800, 9.0%; inpatient rehabilitation facility: 576,700, 1.6%; long-term care hospital: 171,300, 0.5%.
|
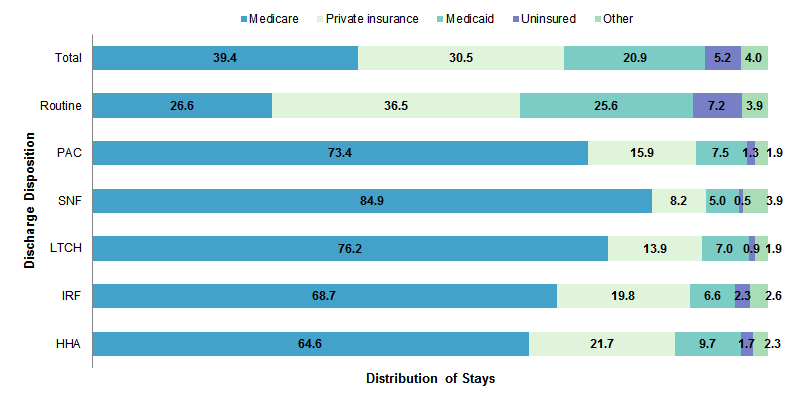
Figure 2 shows the percentage of different primary payers for inpatient stays by discharge disposition. Medicare discharges in this Statistical Brief include both FFS beneficiaries and Medicare Advantage plan enrollees. |
|
Figure 2. Payer mix by discharge disposition, 2013
Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility Figure 2 is a bar chart that shows the distribution of discharges by payer mix for 2013. Total: Medicare: 39.4%, private insurance: 30.5%, Medicaid: 20.9%, uninsured: 5.2%, other: 4.0%. Routine: Medicare: 26.6%, private insurance: 36.5%, Medicaid: 25.6%, uninsured: 7.2%, other: 3.9%. Postacute care: Medicare: 73.4%, private insurance: 15.9%, Medicaid: 7.5%, uninsured: 1.3%, other: 1.9%. Skilled nursing facility: Medicare: 84.9%, private insurance: 8.2%, Medicaid: 5.0%, uninsured: 0.5%, other: 3.9%. Long-term care hospital: Medicare: 76.2%, private insurance: 13.9%, Medicaid: 7.0%, uninsured: 0.9%, other: 1.9%. Inpatient rehabilitation facility: Medicare: 68.7%, private insurance: 19.8%, Medicaid: 6.6%, uninsured: 2.3%, other: 2.6%. Home health agency: Medicare: 64.6%, private insurance: 21.7%, Medicaid: 9.7%, uninsured: 1.7%, other: 2.3%.
|
|
|
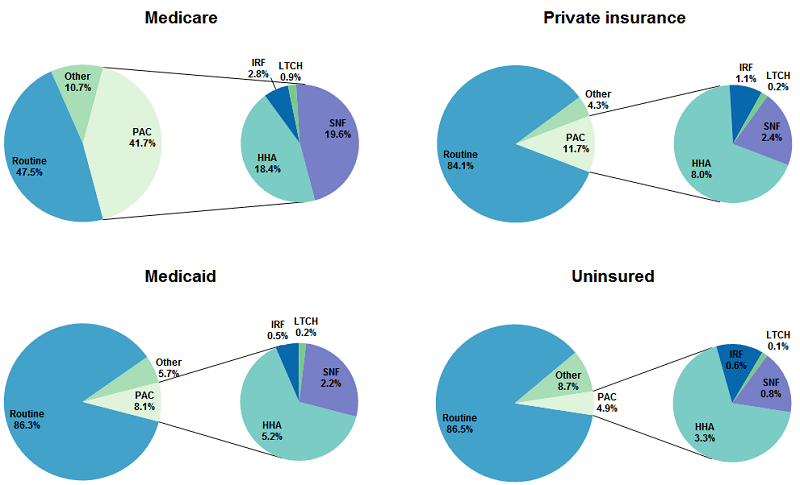
Figure 3. Discharge disposition by payer group, 2013
Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility Figure 3 is made up of four sets of two pie charts, one set for each payer. For each set, one pie chart shows the distribution of discharge disposition between routine, postacute care, and other, and the second pie chart shows the distribution of discharge disposition for stays discharged to postacute care. Medicare: all discharges: routine: 47.5%, postacute care: 41.7%, other: 10.7%; discharges to postacute care: skilled nursing facility: 19.6%, home health agency: 18.4%, inpatient rehabilitation facility: 2.8%, long-term care hospital: 0.9%. Private insurance: all discharges: routine: 84.1%, postacute care: 11.7%, other: 4.3%; discharges to postacute care: home health agency: 8.0%, skilled nursing facility: 2.4%, inpatient rehabilitation facility: 1.1%, long-term care hospital: 0.2%. Medicaid: all discharges: routine: 86.3%, postacute care: 8.1%, other: 5.7%; discharges to postacute care: home health agency: 5.2%, skilled nursing facility: 2.2%, inpatient rehabilitation facility: 0.5%, long-term care hospital: 0.2%. Uninsured: all discharges: routine: 86.5%, other: 8.7%, postacute care: 4.7%; discharges to postacute care: home health agency: 3.3%, skilled nursing facility: 0.8%, inpatient rehabilitation facility: 0.6%, long-term care hospital: 0.1%.
|
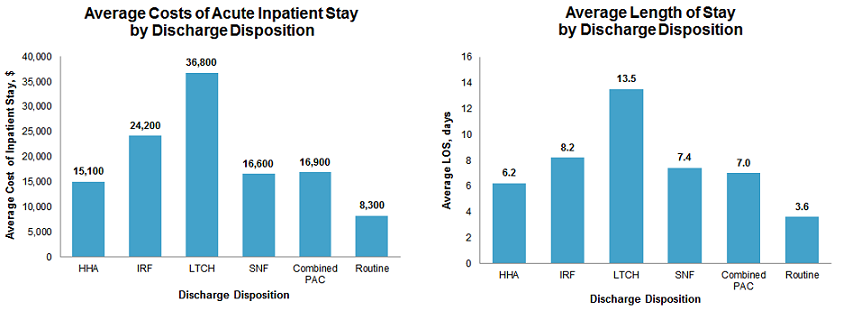
Figure 4 presents the average costs and length of stay of acute care hospital stays by discharge disposition. |
|
Figure 4. Average costs and length of acute care hospital stays by discharge disposition, 2013
Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LOS, length of stay; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility Figure 4 is made up of two bar charts, one for average costs of an acute inpatient stay by discharge disposition and one for average length of stay by discharge disposition. Average cost of inpatient stay: home health agency: $15,100, inpatient rehabilitation facility: $24,200, long-term care hospital: $36,800, skilled nursing facility: $16,600, combined postacute care: $16,900, routine: $8,300. Average length of stay: home health agency: 6.2 days, inpatient rehabilitation facility: 8.2 days, long-term care hospital: 13.5 days, skilled nursing facility: 7.4 days, combined postacute care: 7.0 days, routine: 3.6 days.
|
Table 1 shows patient and hospital characteristics for acute care hospital stays by discharge disposition. |
| Table 1 shows patient and hospital characteristics for acute care hospital stays by discharge disposition. | |||||||
| Characteristics | Discharge disposition | ||||||
|---|---|---|---|---|---|---|---|
| PAC | Routine | ||||||
| Combined PAC | HHA | IRF | LTCH | SNF | |||
| Patient characteristics | |||||||
| Age group years, % | <17 | 1.9 | 3.6 | 0.9 | 0.6 | 0.1 | 21.3 |
| 18-44 | 5.6 | 8.1 | 7.4 | 7.5 | 1.9 | 21.3 | |
| 45-64 | 23.0 | 28.1 | 26.2 | 29.6 | 15.7 | 24.8 | |
| >65 | 69.5 | 60.1 | 65.5 | 62.3 | 82.2 | 22.4 | |
| Sex, % | Male | 42.4 | 43.9 | 46.3 | 50.2 | 39.5 | 41.7 |
| Female | 57.6 | 56.1 | 53.7 | 49.8 | 60.5 | 58.3 | |
| Race, a% | White | 71.4 | 69.7 | 72.6 | 66.1 | 73.6 | 58.4 |
| Black | 12.6 | 13.4 | 13.0 | 17.4 | 11.2 | 14.4 | |
| 6.5 | 7.3 | 5.5 | 7.5 | 5.6 | 13.4 | ||
| Asian | 1.8 | 1.8 | 1.3 | 1.1 | 1.8 | 3.0 | |
| Other | 2.6 | 2.8 | 3.0 | 3.2 | 2.3 | 4.2 | |
| Community-level income, % | 1st quartile (poorest) | 27.5 | 28.1 | 28.7 | 34.3 | 26.0 | 28.8 |
| 2nd quartile | 25.7 | 25.2 | 26.1 | 28.3 | 26.1 | 25.7 | |
| 3rd quartile | 23.9 | 23.6 | 23.8 | 21.9 | 24.4 | 23.7 | |
| 4th quartile (wealthiest) | 21.0 | 21.0 | 19.3 | 13.2 | 21.7 | 19.5 | |
| Hospital characteristics | |||||||
| Hospital teaching status, % | Rural | 10.5 | 10.0 | 6.9 | 7.2 | 11.9 | 10.6 |
| Urban, nonteaching | 38.2 | 36.1 | 34.5 | 39.8 | 41.3 | 36.7 | |
| Urban, teaching | 51.3 | 53.9 | 58.7 | 53.0 | 46.8 | 52.7 | |
| Hospital size, % | Small | 17.3 | 17.2 | 16.0 | 17.1 | 17.5 | 16.4 |
| Medium | 26.1 | 25.6 | 25.4 | 26.7 | 26.9 | 27.0 | |
| Large | 56.6 | 57.2 | 58.6 | 56.2 | 55.6 | 56.6 | |
| Hospital region, % | Northeast | 24.3 | 25.2 | 22.3 | 14.0 | 24.2 | 17.1 |
| Midwest | 23.4 | 22.0 | 22.3 | 27.5 | 25.2 | 22.1 | |
| South | 36.5 | 37.6 | 46.6 | 50.2 | 32.6 | 39.5 | |
| Westb | 15.7 | 15.2 | 8.8 | 8.4 | 18.1 | 21.2 | |
| Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility a About 6 percent all inpatient stays had missing value of race. b Discharges to IRFs and LTCHs were not identified in one State in the West region. As a result, the number of discharges to PAC may be underestimated by 1% with the assumption that the rate of discharge to IRFs and LTCHs in this State is the same as the national rate. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2013 | |||||||
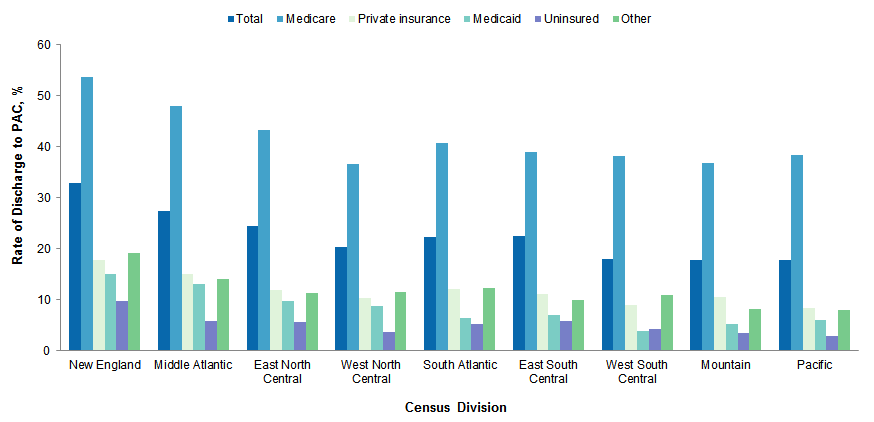
Figure 5 shows the rate of stays discharged to PAC in nine census divisions by payer group. |
|
Figure 5. Rate of discharge to PAC in census divisions by payer, 2013
Abbreviation: PAC, postacute care Figure 5 shows the rate of discharge to postacute care for nine census divisions in 2013 by payer. New England: total: 32.8%, Medicare: 53.6%, Medicaid: 15.2%, private insurance: 17.8%, uninsured: 9.8%, other: 19.2%. Middle Atlantic: total: 27.5%, Medicare: 48.0%, Medicaid: 13.2%, private insurance: 15.1%, uninsured: 5.8%, other: 14.2%. East North Central: total: 24.6%, Medicare; 43.3%, Medicaid: 9.8%, private insurance: 12.0%, uninsured: 5.7%, other: 11.3%. West North Central: total: 20.4%, Medicare; 36.6%, Medicaid: 8.9%, private insurance: 10.4%, uninsured: 3.6%, other: 11.5%. South Atlantic: total: 22.2%, Medicare; 40.8%, Medicaid: 6.5%, private insurance: 12.1%, uninsured: 5.3%, other: 12.3%. East South Central: total: 22.5%, Medicare; 39.0%, Medicaid: 7.1%, private insurance: 11.1%, uninsured: 5.8%, other: 10.0%. West South Central: total: 18.0%, Medicare; 38.2%, Medicaid: 3.9%, private insurance: 9.0%, uninsured: 4.3%, other: 11.0%. Mountain: total: 17.8%, Medicare; 36.8%, Medicaid: 5.3%, private insurance: 10.6%, uninsured: 3.5%, other: 8.3%. Pacific: total: 17.8%, Medicare; 38.5%, Medicaid: 6.1%, private insurance: 8.4%, uninsured: 2.9%, other: 8.1%.
|
Only 4 out of 751 MS-DRG groups did not have any stays with discharges to PAC; however, the top 10 MS-DRGs accounted for 37 percent of all discharges to PAC settings. Table 2 displays the top 10 conditions and procedures with the most discharges to PAC, the number and rate of discharge to PAC for these conditions and procedures, and number and rate of discharge to each type of PAC. |
| Table 2. Top 10 conditions and procedures with discharges to PAC, 2013 | ||||||||||||
| Conditions/procedures | Total discharges to PAC | Discharges to PAC setting | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HHA | IRF | LTCH | SNF | |||||||||
| n | % | n | % | n | % | n | % | n | % | |||
| Total hip/knee joint replacement (MS-DRG 469, 470) | 755,700 | 70.7 | 409,000 | 54.1 | 63,500 | 8.4 | 1,300 | 0.2 | 282,000 | 37.3 | ||
| Septicemia or severe sepsis (MS-DRG 870-872) | 441,400 | 39.4 | 172,500 | 39.1 | 15,200 | 3.4 | 17,700 | 4.0 | 236,000 | 53.5 | ||
| Heart failure & shock (MS-DRG 291-293) | 334,800 | 40.6 | 194,400 | 58.1 | 9,000 | 2.7 | 4,300 | 1.3 | 127,100 | 38.0 | ||
| Stroke (MS-DRG 61-66) | 247,400 | 47.9 | 65,500 | 26.5 | 80,700 | 32.6 | 2,300 | 0.9 | 99,000 | 40.0 | ||
| Simple pneumonia & pleurisy (MS-DRG 193-195) | 246,500 | 28.3 | 119,100 | 48.3 | 7,000 | 2.8 | 4,100 | 1.7 | 116,300 | 47.2 | ||
| Renal failure (MS-DRG 682-684) | 204,700 | 36.4 | 91,800 | 44.9 | 7,100 | 3.4 | 3,200 | 1.5 | 102,600 | 50.1 | ||
| Kidney & urinary tract infection (MS-DRG 689-690) | 199,500 | 39.2 | 78,800 | 39.5 | 5,800 | 2.9 | 2,100 | 1.1 | 112,900 | 56.6 | ||
| Chronic obstructive pulmonary disease (MS-DRG 190-192) | 197,500 | 27.0 | 125,700 | 63.6 | 4,700 | 2.4 | 2,700 | 1.4 | 64,500 | 32.6 | ||
| Hip & femur procedure except major joint (MS-DRG 480-482) | 186,300 | 75.7 | 24,700 | 13.3 | 31,800 | 17.1 | 1,300 | 0.7 | 128,400 | 68.9 | ||
| Cellulitis (MS-DRG 602, 603) | 127,500 | 24.1 | 78,600 | 61.6 | 2,630 | 2.1 | 2,500 | 1.9 | 43,800 | 34.4 | ||
| All discharges in top 10 conditions/procedures | 2,941,400 | 41.2 | 1,360,100 | 46.3 | 227,300 | 7.7 | 41,500 | 1.4 | 1,312,500 | 44.6 | ||
| All discharges to PAC, % | 37.0 | - | 34.1 | - | 39.4 | - | 24.2 | - | 40.7 | - | ||
| Abbreviations: HHA, home health agency; IRF, inpatient rehabilitation facility; LTCH, long-term care hospital; PAC, postacute care; SNF, skilled nursing facility Note: Approximately 174,000 rehabilitation (MS-DRG 945, 946) stays were discharged to PAC. These cases were not included here because they are considered PAC stays rather than acute inpatient stays. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2013 | ||||||||||||
Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) 2013 Nationwide Inpatient Sample (NIS). Information on discharge to postacute care was obtained from intramural data that is specific to each State and that required State-specific and year-specific algorithms to generate a measure of discharge status that was comparable across States. Supplemental sources included population denominator data for use with HCUP databases, derived from information available from the Bureau of the Census.6 Many hypothesis tests were conducted for this Statistical Brief. Thus, to decrease the number of false-positive results, we reduced the significance level to .01 for individual tests. Definitions Diagnosis-related groups (DRGs) DRGs comprise a patient classification system that categorizes patients into groups that are clinically coherent and homogeneous with respect to resource use. DRGs group patients according to diagnosis, type of treatment (procedure), age, and other relevant criteria. Each hospital stay has one assigned DRG. Types of discharge destinations The definitions of discharges to PAC and routine discharges are:
The National Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Costs and charges Total hospital charges were converted to costs using HCUP Cost-to-Charge Ratios based on hospital accounting reports from the Centers for Medicare & Medicaid Services (CMS).7 Costs reflect the actual expenses incurred in the production of hospital services, such as wages, supplies, and utility costs; charges represent the amount a hospital billed for the case. For each hospital, a hospital-wide cost-to-charge ratio is used. Hospital charges reflect the amount the hospital billed for the entire hospital stay and do not include professional (physician) fees. For the purposes of this Statistical Brief, costs are reported to the nearest hundred. How HCUP estimates of costs differ from National Health Expenditure Accounts There are a number of differences between the costs cited in this Statistical Brief and spending as measured in the National Health Expenditure Accounts (NHEA), which are produced annually by CMS.8 The largest source of difference comes from the HCUP coverage of inpatient treatment only in contrast to the NHEA inclusion of outpatient costs associated with emergency departments and other hospital-based outpatient clinics and departments as well. The outpatient portion of hospitals' activities has been growing steadily and may exceed half of all hospital revenue in recent years. On the basis of the American Hospital Association (AHA) Annual Survey, 2012 outpatient gross revenues (or charges) were about 44 percent of total hospital gross revenues.9 Smaller sources of differences come from the inclusion in the NHEA of hospitals that are excluded from HCUP. These include Federal hospitals (Department of Defense, Veterans Administration, Indian Health Services, and Department of Justice [prison] hospitals) as well as psychiatric, substance abuse, and long-term care hospitals. A third source of difference lies in the HCUP reliance on billed charges from hospitals to payers, adjusted to provide estimates of costs using hospital-wide cost-to-charge ratios, in contrast to the NHEA measurement of spending or revenue. HCUP costs estimate the amount of money required to produce hospital services, including expenses for wages, salaries, and benefits paid to staff as well as utilities, maintenance, and other similar expenses required to run a hospital. NHEA spending or revenue measures the amount of income received by the hospital for treatment and other services provided, including payments by insurers, patients, or government programs. The difference between revenues and costs include profit for for-profit hospitals or surpluses for nonprofit hospitals. Hospital location/teaching status Hospital urban/rural designation was based on the Core Based Statistical Area (CBSA). Hospitals residing in counties with a CBSA type of metropolitan were considered urban, while hospitals with a CBSA type of micropolitan or non-core were classified as rural. SA hospital is considered to be a teaching hospital if it has a residency program approved by the American Medical Association (AMA), is a member of the Council of Teaching Hospitals (COTH), or has a ratio of full-time equivalent interns and residents to beds of .25 or higher. Rural hospitals were not split according to teaching status because rural teaching hospitals were rare. Hospital bed size Hospital bed size categories are based on hospital beds and are specific to the hospital's location and teaching status (see Table 3). Bed size assesses the number of short-term acute beds in a hospital. Hospital information was obtained from the AHA Annual Survey of Hospitals. |
| Table 3. Hospital bed size categories | |||
| Location and teaching status | Hospital bed size | ||
|---|---|---|---|
| Small | Medium | Large | |
| Northeast region | |||
| Rural | 1-49 | 50-99 | 100+ |
| Urban, nonteaching | 1-124 | 125-199 | 200+ |
| Urban, teaching | 1-249 | 250-424 | 425+ |
| Midwest region | |||
| Rural | 1-29 | 30-49 | 50+ |
| Urban, nonteaching | 1-74 | 75-174 | 175+ |
| Urban, teaching | 1-249 | 250-374 | 375+ |
| Southern region | |||
| Rural | 1-39 | 40-74 | 75+ |
| Urban, nonteaching | 1-99 | 100-199 | 200+ |
| Urban, teaching | 1-249 | 250-449 | 450+ |
| Western region | |||
| Rural | 1-24 | 25-44 | 45+ |
| Urban, nonteaching | 1-99 | 100-174 | 175+ |
| Urban, teaching | 1-199 | 200-324 | 325+ |
Median community-level income Median community-level income is the median household income of the patient's ZIP Code of residence. Income levels are separated into population-based quartiles with cut-offs determined using ZIP Code demographic data obtained from the Nielsen Company. Patients in the first quartile are designated as having low income, and patients in the upper three quartiles are designated as having not low income. The income quartile is missing for patients who are homeless or foreign. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Region Region is one of the four regions defined by the U.S. Census Bureau:
Census division is one of the nine divisions defined by the U.S. Census Bureau:10
Data on Hispanic ethnicity are collected differently among the States and also can differ from the Census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other (including mixed race)) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, Asian/Pacific Islander, and non-Hispanic Other. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health and Hospitals Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About Statistical Briefs HCUP Statistical Briefs are descriptive summary reports presenting statistics on hospital inpatient and emergency department use and costs, quality of care, access to care, medical conditions, procedures, patient populations, and other topics. The reports use HCUP administrative healthcare data. About the NIS The HCUP National Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
About the HCUPnet HCUPnet is an online query system that offers instant access to the largest set of all-payer healthcare databases that are publicly available. HCUPnet has an easy step-by-step query system that creates tables and graphs of national and regional statistics as well as data trends for community hospitals in the United States. HCUPnet generates statistics using data from HCUP's National (Nationwide) Inpatient Sample (NIS), the Kids' Inpatient Database (KID), the Nationwide Emergency Department Sample (NEDS), the Nationwide Readmissions Database (NRD), the State Inpatient Databases (SID), and the State Emergency Department Databases (SEDD). For More Information For more information about HCUP, visit http://www.hcup-us.ahrq.gov/. For additional HCUP statistics, visit HCUP Fast Stats at https://datatools.ahrq.gov/hcup-fast-stats for easy access to the latest HCUP-based statistics for health information topics, or visit HCUPnet, our interactive query system, at https://datatools.ahrq.gov/hcupnet. For information on other hospitalizations in the United States, refer to the following HCUP Statistical Briefs located at http://www.hcup-us.ahrq.gov/reports/statbriefs/statbriefs.jsp:
For a detailed description of HCUP and more information on the design of the National Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2015. http://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 17, 2016. Suggested Citation Tian W. (AHRQ). An All-Payer View of Hospital Discharge to Postacute Care, 2013. HCUP Statistical Brief #205. May 2016. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb205-Hospital-Discharge-Postacute-Care.pdf. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:David Knutson, Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 1 Medicare Payment Advisory Commission. Health Care Spending and the Medicare Program. MedPAC Annual Data Book. Section 8: Post-Acute Care. Washington, DC: Medicare Payment Advisory Commission; June 2015. 2 American Hospital Association. TrendWatch: Maximizing the Value of Post-Acute Care. Washington, DC: American Hospital Association; November 2010. 3 Medicare Payment Advisory Commission. Report to the Congress: Medicare Payment Policy. Chapter 7: Medicare's Post-Acute Care: Trends and Ways to Rationalize Payments. Washington, DC: Medicare Payment Advisory Commission; March 2015. 4 Medicare Payment Advisory Commission. Health Care Spending and the Medicare Program. Op. cit. 5 Buntin MB, Garten AD, Paddock S, Saliba D, Totten M, Escarce JJ. How much is post-acute care use affected by its availability? Health Services Research. 2005;40(2):413-34. 6 Barrett M, Hickey K, Coffey R, Levit K. Population Denominator Data for Use with the HCUP Databases (Updated with 2014 Population Data). HCUP Methods Series Report #2015-07. September 1, 2015. U.S. Agency for Healthcare Research and Quality. http://www.hcup-us.ahrq.gov/reports/methods/2015-07.pdf. Accessed February 17, 2016. 7 Agency for Healthcare Research and Quality. HCUP Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). 2001-2013. Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2015. http://www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed February 17, 2016. 8 For additional information about the NHEA, see Centers for Medicare & Medicaid Services (CMS). National Health Expenditure Data. CMS website May 2014. http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/index.html?redirect=/NationalHealthExpendData/. Accessed February 17, 2016. 9 American Hospital Association. TrendWatch Chartbook, 2014. Table 4.2. Distribution of Inpatient vs. Outpatient Revenues, 1992-2012. https://www.aha.org/system/files/research/reports/tw/chartbook/2016/2016chartbook.pdf. 10 U.S. Census Bureau. Census Regions and Divisions of the United States. https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf. Accessed November 8, 2017. |
| Internet Citation: Statistical Brief #205. Healthcare Cost and Utilization Project (HCUP). June 2016. Agency for Healthcare Research and Quality, Rockville, MD. hcup-us.ahrq.gov/reports/statbriefs/sb205-Hospital-Discharge-Postacute-Care.jsp. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| If you are experiencing issues related to Section 508 accessibility of information on this website, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 6/23/16 |