STATISTICAL BRIEF #215 |
December 2016
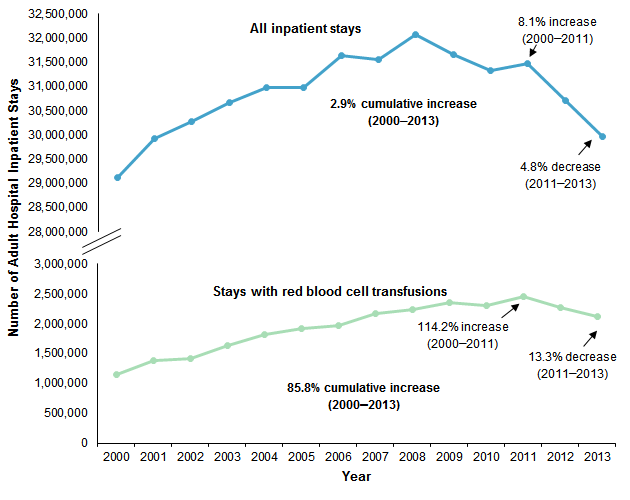
Kamille A. West, M.D., Marguerite L. Barrett, M.S., Brian J. Moore, Ph.D., Jeffery L. Miller, M.D., and Claudia A. Steiner, M.D., M.P.H. Introduction Blood transfusion is a medical procedure to supply blood and blood components to a patient through an intravenous line in order to replace blood lost during surgery or injury, or when the body cannot make blood properly because of illness.1 In modern practice, blood is separated into components to meet the specific needs of the patient. Red blood cells are the most commonly transfused blood component. Although blood transfusion is recognized as crucial in treating certain diseases or conditions, published guidelines on blood utilization recommend restricting red blood cell transfusion in hospitalized patients to minimize adverse outcomes and reduce unnecessary healthcare costs.2 National surveys have reported an overall decrease in the number of units of blood transfused in inpatient and outpatient settings.3,4 However, a recent brief report demonstrated an increase in blood transfusions per inpatient hospital stay.5 As suggested in a recent study, analyses that further describe the patient populations receiving blood transfusions will help inform and improve the use of blood transfusions, specifically red cells, and improve costs and resource use in hospitals.6 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents national data on hospital inpatient stays among adults with a red blood cell transfusion from 2000 to 2013. The analyses focus on stays with any red blood cell transfusion, rather than on the number of blood units transfused. We present trends in stays with a red blood cell transfusion relative to the trend in all inpatient stays from 2000 to 2013 as well as an overview of characteristics of stays with a red blood cell transfusion. We also present trends in the percentage of stays with a red blood cell transfusion by age. We then focus on 2013 and present the most frequent diagnoses for stays with a red blood cell transfusion. In addition, we examine the most commonly performed procedures that occur among patients receiving a red blood cell transfusion. All differences noted in the text differ by at least 10 percent. Findings Trends in inpatient stays with a red blood cell transfusion, 2000-2013 Figure 1 presents the total number of adult inpatient stays and the number of stays with a red blood cell transfusion from 2000 through 2013. |
|
|
Figure 1. Trends in inpatient hospitalizations and hospitalizations with a red blood cell transfusion for adults, 2000-2013
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000-2013 Line graph showing the number of all inpatient adult hospital inpatient stays and those with a red blood cell transfusion. All inpatient stays: 2000, 29,126,053; 2001, 29,920,995; 2002, 30,268,725; 2003, 30,676,256; 2004, 30,966,846; 2005, 30,978,228; 2006, 31,628,376; 2007, 31,551,163; 2008, 32,060,332; 2009, 31,647,642; 2010, 31,318,051; 2011, 31,472,521; 2012, 30,712,524; 2013, 29,969,451, for a cumulative increase of 2.9%. Stays with a red blood cell transfusion: 2000, 1,141,495; 2001, 1,386,036; 2002, 1,422,962; 2003, 1,635,534; 2004, 1,815,566; 2005, 1,919,872; 2006, 1,961,628; 2007, 2,168,151; 2008, 2,242,831; 2009, 2,344,304; 2010, 2,302,865; 2011, 2,445,549; 2012, 2,275,330; 2013, 2,120,739, for a cumulative increase of 85.8%.
|
Characteristics of hospital inpatient stays with a red blood cell transfusion, 2000-2013 Table 1 presents patient and hospital stay characteristics for inpatient hospitalizations with a red blood cell transfusion in 2000 and 2013. |
| Table 1. Characteristics of adult inpatient hospitalizations with a red blood cell transfusion, 2000 and 2013 | ||
| Characteristics | 2000 | 2013 |
|---|---|---|
| Number of stays | 1,141,500 | 2,120,700 |
| Percentage of total inpatient stays | 3.9 | 7.1 |
| Patient characteristics | ||
| Age, years, mean | 67.5 | 65.7 |
| Age, years, % | ||
| 18-44 | 12.9 | 13.1 |
| 45-64 | 22.9 | 28.5 |
| 65+ | 64.3 | 58.4 |
| Sex, % | ||
| Female | 58.0 | 57.2 |
| Male | 42.0 | 42.8 |
| Expected primary payer, % | ||
| Medicare | 63.3 | 62.7 |
| Medicaid | 8.8 | 10.9 |
| Private insurance | 21.7 | 19.6 |
| Uninsured | 3.6 | 4.2 |
| Other | 2.1 | 2.5 |
| Region, rate per 100,000 adults | ||
| Northeast | 638.9 | 939.8 |
| Midwest | 328.8 | 784.3 |
| South | 661.4 | 1,005.6 |
| West | 498.1 | 733.5 |
| Hospital stay characteristics | ||
| Length of stay, mean, days | 8.9 | 8.3 |
| Total hospital costs, mean, $a | 19,000 | 23,300 |
| Admissions from the ED, % | 51.9 | 63.3 |
| Abbreviation: ED, emergency department a Hospital costs in 2000 are inflation adjusted and expressed in 2013 dollars. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 | ||
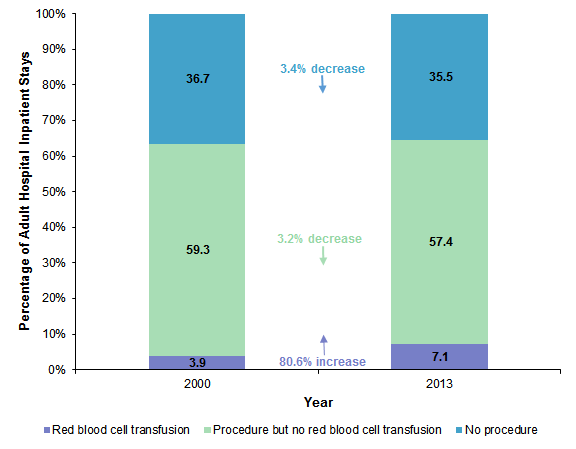
Figure 2 presents the distribution of hospital inpatient stays with a red blood cell transfusion, with another procedure but no red blood cell transfusion, or with no procedure in 2000 and 2013. |
|
Figure 2. Change in the percentage of adult inpatient stays by type of procedure, 2000 and 2013
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 Stacked bar chart showing the percentage of inpatient stays by procedure type for 2000 and 2013. No procedure: 2000, 36.7%; 2013, 35.5%—a 3.4% decrease. Procedure but no red blood cell transfusion: 2000, 59.3%; 2013, 57.4%—a 3.2% decrease. Red blood cell transfusion: 2000, 3.9%; 2013, 7.1%—an 80.6% increase.
|
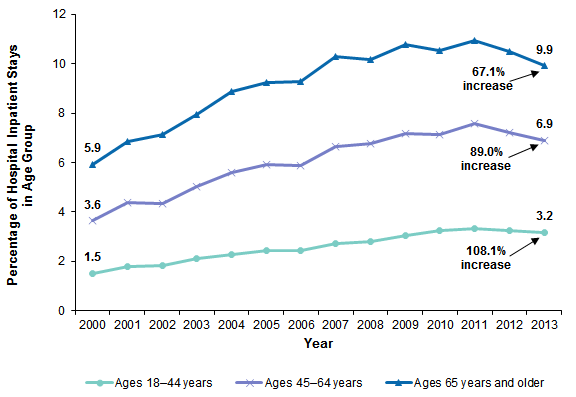
Figure 3 presents trends in stays with a red blood cell transfusion as a percentage of total hospital inpatient stays, by patient age, from 2000 through 2013. |
|
Figure 3. Trends in the percentage of adult inpatient hospitalizations with a red blood cell transfusion by patient age, 2000-2013
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000-2013 Line drawing showing the percentage of adult inpatient hospitalizations with a red blood cell transfusion by age, 2000-2012. Ages 18-44 years: 2000, 1.5; 2001, 1.8; 2002, 1.8; 2003, 2.1; 2004, 2.3; 2005, 2.4; 2006, 2.4; 2007, 2.7; 2008, 2.8; 2009, 3.1; 2010, 3.2; 2011, 3.3; 2012, 3.2; 2013, 3.2. Ages 45-64 years: 2000, 3.6; 2001, 4.4; 2002, 4.3; 2003, 5.0; 2004, 5.6; 2005, 5.9; 2006, 5.9; 2007, 6.7; 2008, 6.8; 2009, 7.2; 2010, 7.2; 2011, 7.6; 2012, 7.2; 2013, 6.9. Ages 65+ years: 2000, 5.9; 2001, 6.9; 2002, 7.1; 2003, 8.0; 2004, 8.9; 2005, 9.2; 2006, 9.3; 2007, 10.3; 2008, 10.2; 2009, 10.8; 2010, 10.5; 2011, 10.9; 2012, 10.5; 2013, 9.9.
|
Reasons for hospitalizations of adults with a red blood cell transfusion, 2000 and 2013 Table 2 lists the 15 most frequent principal diagnoses among hospitalizations with a red blood cell transfusion in 2013. Data on the same diagnoses also are provided for 2000 for comparison. |
| Table 2. Top 15 conditions with a red blood cell transfusion in 2013, compared with the frequency of each condition in 2000 | ||||||
| Principal conditions | 2000 | 2013 | ||||
|---|---|---|---|---|---|---|
| Stays with red blood cell transfusion | Total stays | Stays with red blood cell transfusion | Total stays | |||
| N | % | N | N | % | N | |
| Septicemia (except in labor) | 28,603 | 9.3 | 308,638 | 174,740 | 13.7 | 1,276,805 |
| Gastrointestinal hemorrhage | 105,171 | 32.3 | 326,074 | 171,995 | 47.6 | 361,375 |
| Hereditary, nutritional, hemolytic, and bone marrow failure anemias | 68,000 | 51.7 | 131,595 | 141,225 | 73.2 | 192,885 |
| Fracture of neck of femur (hip) | 59,144 | 19.5 | 302,890 | 87,590 | 29.1 | 301,190 |
| Complication of device; implant or graft | 33,950 | 6.9 | 489,383 | 81,865 | 13.4 | 608,920 |
| Osteoarthritis | 36,177 | 8.4 | 430,281 | 79,410 | 7.8 | 1,022,945 |
| Acute and unspecified renal failure | 13,695 | 11.3 | 121,451 | 54,830 | 11.1 | 495,000 |
| Complications of surgical procedures or medical care | 19,859 | 5.6 | 357,398 | 52,205 | 11.7 | 447,230 |
| Congestive heart failure; nonhypertensive | 36,712 | 3.7 | 992,426 | 49,365 | 5.6 | 880,629 |
| Pneumonia (except that caused by tuberculosis or sexually transmitted disease) | 43,914 | 4.1 | 1,061,987 | 48,840 | 5.7 | 862,234 |
| Acute myocardial infarction | 31,687 | 4.3 | 744,848 | 38,565 | 6.4 | 602,235 |
| Diverticulosis and diverticulitis | 27,189 | 10.3 | 263,459 | 37,885 | 12.8 | 295,955 |
| Coronary atherosclerosis and other heart disease | 40,141 | 3.0 | 1,316,200 | 32,440 | 7.1 | 458,295 |
| Acute posthemorrhagic anemia | 5,443 | 52.6 | 10,340 | 31,485 | 75.6 | 41,650 |
| Heart valve disorders | 8,339 | 9.9 | 84,139 | 27,800 | 22.8 | 121,825 |
| Note: Table is sorted by the highest number of stays with a red blood cell transfusion in 2013. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 | ||||||
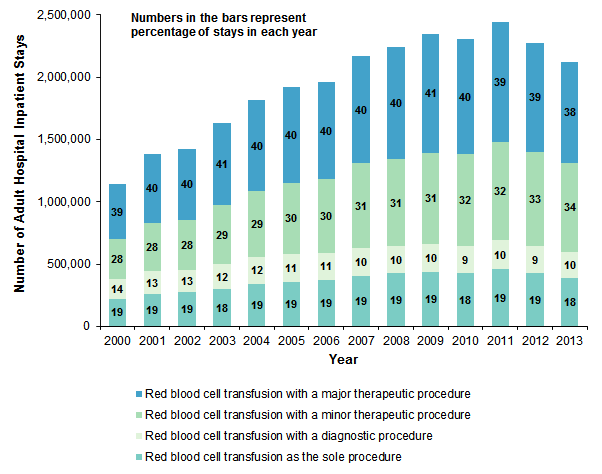
Figure 4 presents the distribution of stays with a red blood cell transfusion occurring with and without another procedure performed. For stays during which another procedure occurred, the procedures are categorized into three broad categories—major therapeutic, minor therapeutic, and diagnostic. |
|
Figure 4. Trends in adult inpatient hospitalizations with a red blood cell transfusion by type of procedure, 2000-2013
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000-2013 Stacked bar chart showing percentage of stays each year by type of red blood cell transfusion procedure, 2000-2013. 2000: with a major therapeutic procedure, 39; with a minor therapeutic procedure, 28; with a diagnostic procedure, 14; as the sole procedure, 19. 2001: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 28; with a diagnostic procedure, 13; as the sole procedure, 19. 2002: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 28; with a diagnostic procedure, 13; as the sole procedure, 19. 2003: with a major therapeutic procedure, 41; with a minor therapeutic procedure, 29; with a diagnostic procedure, 12; as the sole procedure, 18. 2004: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 29; with a diagnostic procedure, 12; as the sole procedure, 19. 2005: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 30; with a diagnostic procedure, 11; as the sole procedure, 19. 2006: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 30; with a diagnostic procedure, 11; as the sole procedure, 19. 2007: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 31; with a diagnostic procedure, 10; as the sole procedure, 19. 2008: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 31; with a diagnostic procedure, 10; as the sole procedure, 19. 2009: with a major therapeutic procedure, 41; with a minor therapeutic procedure, 31; with a diagnostic procedure, 10; as the sole procedure, 19. 2010: with a major therapeutic procedure, 40; with a minor therapeutic procedure, 32; with a diagnostic procedure, 9; as the sole procedure, 18. 2011: with a major therapeutic procedure, 39; with a minor therapeutic procedure, 32; with a diagnostic procedure, 10; as the sole procedure, 19. 2012: with a major therapeutic procedure, 39; with a minor therapeutic procedure, 33; with a diagnostic procedure, 9; as the sole procedure, 19. 2013: with a major therapeutic procedure, 38; with a minor therapeutic procedure, 34; with a diagnostic procedure, 10; as the sole procedure, 18.
|
In each year, about 19 percent of inpatient stays with a red blood cell transfusion involved no other procedure. Table 3 lists the 15 most frequent principal diagnoses among hospitalizations with a red blood cell transfusion as the sole procedure in 2013. Data on the same diagnoses also are provided for 2000 for comparison. |
| Table 3. Top 15 conditions with a red blood cell transfusion as the sole procedure in 2013, compared with the frequency of each condition in 2000 | ||||||
| Principal condition | 2000 | 2013 | ||||
|---|---|---|---|---|---|---|
| Stays with red blood cell transfusion as the sole procedure | Total stays | Stays with red blood cell transfusion as the sole procedure | Total stays | |||
| N | % | N | N | % | N | |
| Hereditary, nutritional, hemolytic, and bone marrow failure anemias | 39,269 | 29.8 | 131,595 | 75,585 | 39.2 | 192,885 |
| Septicemia (except in labor) | 7,345 | 2.4 | 308,638 | 27,050 | 2.1 | 1,276,805 |
| Gastrointestinal hemorrhage | 16,394 | 5.0 | 326,074 | 19,630 | 5.4 | 361,375 |
| Acute and unspecified renal failure | 3,340 | 2.7 | 121,451 | 19,490 | 3.9 | 495,000 |
| Pneumonia (except that caused by tuberculosis or sexually transmitted disease) | 16,275 | 1.5 | 1,061,987 | 18,795 | 2.2 | 862,234 |
| Congestive heart failure; nonhypertensive | 15,306 | 1.5 | 992,426 | 18,715 | 2.1 | 880,629 |
| Sickle cell anemia | 6,893 | 12.2 | 56,425 | 17,240 | 24.0 | 71,755 |
| Acute posthemorrhagic anemia | 3,161 | 30.6 | 10,340 | 14,270 | 34.3 | 41,650 |
| Urinary tract infections | 5,661 | 1.5 | 378,025 | 8,950 | 1.8 | 490,099 |
| Complications of surgical procedures or medical care | 3,268 | 0.9 | 357,398 | 8,695 | 1.9 | 447,230 |
| Fluid and electrolyte disorders | 7,053 | 1.7 | 419,688 | 6,685 | 1.8 | 362,335 |
| Chronic obstructive pulmonary disease and bronchiectasis | 3,329 | 0.6 | 596,096 | 6,425 | 1.0 | 642,224 |
| Diseases of white blood cells | 3,055 | 8.3 | 36,612 | 6,230 | 12.3 | 50,555 |
| Diverticulosis and diverticulitis | 3,554 | 1.3 | 263,459 | 5,780 | 2.0 | 295,955 |
| Acute myocardial infarction | 6,383 | 0.9 | 744,848 | 5,050 | 0.8 | 602,235 |
| Note: Table is sorted by the highest number of stays with a red blood cell transfusion as the sole procedure in 2013. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 | ||||||
In each year, about 40 percent of hospital inpatient stays with a red blood cell transfusion involved a major therapeutic procedure. Table 4 lists the 10 most common major therapeutic procedures in 2013 among hospitalizations with a red blood cell transfusion. Data on the same procedures also are provided for 2000 for comparison. |
| Table 4. Ten most frequent major therapeutic procedure categories for hospital inpatient stays with a red blood cell transfusion in 2013, compared with the frequency of each procedure in 2000 | ||||||
| Procedure category | 2000 | 2013 | ||||
|---|---|---|---|---|---|---|
| Stays with red blood cell transfusion | Total stays | Stays with red blood cell transfusion | Total stays | |||
| N | % | N | N | % | N | |
| Treatment, fracture or dislocation of hip and femur | 53,472 | 21.5 | 248,765 | 91,835 | 33.9 | 271,195 |
| Hip replacement, total and partial | 46,587 | 15.6 | 298,351 | 80,405 | 16.3 | 493,360 |
| Arthroplasty knee | 25,354 | 58.1 | 312,332 | 56,460 | 7.7 | 731,410 |
| Coronary artery bypass graft (CABG) | 43,161 | 11.3 | 383,153 | 49,995 | 25.0 | 199,895 |
| Colorectal resection | 33,017 | 11.7 | 283,076 | 48,900 | 16.4 | 297,500 |
| Heart valve procedures | 11,158 | 13.3 | 84,047 | 36,945 | 28.6 | 129,185 |
| Excision, lysis peritoneal adhesions | 17,654 | 5.4 | 328,580 | 36,280 | 11.3 | 321,075 |
| Partial excision bone | 10,802 | 4.8 | 223,965 | 32,900 | 10.0 | 330,085 |
| Amputation of lower extremity | 17,190 | 13.2 | 130,202 | 28,285 | 20.8 | 135,705 |
| Spinal fusion | 9,336 | 4.0 | 235,775 | 27,740 | 6.3 | 442,610 |
| Note: Table is sorted by highest number of stays with a red blood cell transfusion in 2013 Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 | ||||||
In 2013, approximately 34 percent of inpatient stays with a red blood cell transfusion involved another minor therapeutic procedure. Table 5 lists the 10 most common procedure categories for the minor therapeutic procedures in 2013 among hospitalizations with a red blood cell transfusion. Data on the same procedures also are provided for 2000 for comparison. |
| Table 5. Ten most frequent minor therapeutic procedures for hospital inpatient stays with a red blood cell transfusion in 2013, compared with the frequency of each procedure in 2000 | ||||||
| Procedure category | 2000 | 2013 | ||||
|---|---|---|---|---|---|---|
| Stays with red blood cell transfusion | Total stays | Stays with red blood cell transfusion | Total stays | |||
| N | % | N | N | % | N | |
| Respiratory intubation and mechanical ventilation | 52,855 | 10.1 | 525,643 | 150,440 | 13.9 | 1,080,095 |
| Hemodialysis | 39,600 | 10.8 | 366,945 | 117,630 | 19.0 | 618,525 |
| Enteral and parenteral nutrition | 24,136 | 15.3 | 158,062 | 49,625 | 21.4 | 232,090 |
| Incision of pleura, thoracentesis, chest drainage | 17,794 | 7.3 | 243,931 | 42,160 | 13.4 | 315,460 |
| Abdominal paracentesis | 11,877 | 11.5 | 102,955 | 40,060 | 17.1 | 234,020 |
| Cancer chemotherapy | 17,343 | 9.2 | 187,991 | 35,540 | 20.4 | 174,430 |
| Gastrostomy, temporary and permanent | 11,842 | 8.8 | 134,495 | 19,340 | 16.3 | 118,345 |
| Conversion of cardiac rhythm | 8,084 | 5.6 | 145,148 | 19,045 | 9.9 | 191,725 |
| Indwelling catheter | 2,715 | 8.5 | 31,897 | 17,680 | 12.7 | 139,405 |
| Prophylactic vaccinations and inoculations | 233 | 1.0 | 23.931 | 16.170 | 5.0 | 320,680 |
| Note: Table sorted by highest number of stays with a red blood cell transfusion in 2013 Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2000 and 2013 | ||||||
Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS), 2013. Historical data were drawn from the 2000-2012 National (Nationwide) Inpatient Sample (NIS). Supplemental sources included population denominator data for use with HCUP databases, derived from information available from Nielsen.7 All differences noted in the text differ by at least 10 percent. Definitions Diagnoses, procedures, ICD-9-CM, Procedure Classes, and Clinical Classifications Software (CCS) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. All-listed procedures include all procedures performed during the hospital stay, whether for definitive treatment or for diagnostic or exploratory purposes. The first-listed procedure is the procedure that is listed first on the discharge record. Inpatient data define this as the principal procedure—the procedure that is performed for definitive treatment rather than for diagnostic or exploratory purposes (i.e., the procedure that was necessary to take care of a complication). The term procedure in this Statistical Brief included surgeries as well as minor procedures. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses and procedures. There are approximately 14,000 ICD-9-CM diagnosis codes. There are approximately 4,000 ICD-9-CM procedure codes. The Procedure Classes provide users with an easy way to categorize procedure codes into one of four broad groups: minor diagnostic, minor therapeutic, major diagnostic, and major therapeutic.8 The Procedure Classes are based on the ICD-9-CM codes. For this Statistical Brief, the major and minor diagnostic procedure classes were combined into one category, diagnostic. Each inpatient stay with a red blood cell transfusion was categorized into a single Procedure Class using all-listed procedures (i.e., the principal procedure and up to 14 secondary procedures). The assignment was based on a hierarchy that first looked for the presence of a major therapeutic procedure, then a minor therapeutic procedure, then diagnostic procedures, and finally stays in which red blood cell transfusion was the sole procedure. CCS categorizes ICD-9-CM diagnosis codes and procedure codes into a manageable number of clinically meaningful categories.9 This clinical grouper makes it easier to quickly understand patterns of diagnoses and procedure use. CCS was used to define diagnosis conditions and procedure categories in Tables 2-5. Three categories of anemias from the CCS diagnosis categorization scheme are specifically defined below to clarify the different types of conditions included in each category. Hereditary, nutritional, hemolytic, and bone marrow failure anemias (CCS 59 Deficiency and other anemia) includes ICD-9-CM diagnosis codes: 280.0 280.1 280.8 280.9 281.0 281.1 281.2 281.3 281.4 281.8 281.9 282.0 282.1 282.2 282.3 282.4 282.40 282.43 282.44 282.45 282.46 282.47 282.49 282.7 282.8 282.9 283.0 283.1 283.10 283.11 283.19 283.2 283.9 284.0 284.01 284.09 284.1 284.11 284.12 284.19 284.2 284.8 284.81 284.89 284.9 285.0 285.21 285.22 285.29 285.8 285.9. Acute posthemorrhagic anemia (CCS 60) includes ICD-9-CM diagnosis code: 285.1. Sickle cell anemia (CCS 61) includes ICD-9-CM diagnosis codes: 282.41 282.42 282.5 282.60 282.61 282.62 282.63 282.64 282.68 282.69. Case definition The ICD-9-CM procedure code defining red blood cell transfusion is 99.04, Transfusion of packed cells. For the purposes of this Statistical Brief, we identify any stay with a red blood cell transfusion and do not distinguish the number of blood units used during each stay, which could be one or more than one. Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Costs and charges Total hospital charges were converted to costs using HCUP Cost-to-Charge Ratios based on hospital accounting reports from the Centers for Medicare & Medicaid Services (CMS).10 Costs reflect the actual expenses incurred in the production of hospital services, such as wages, supplies, and utility costs; charges represent the amount a hospital billed for the case. For each hospital, a hospital-wide cost-to-charge ratio is used. Hospital charges reflect the amount the hospital billed for the entire hospital stay and do not include professional (physician) fees. For the purposes of this Statistical Brief, costs are reported to the nearest hundred. Annual costs were inflation adjusted using the Gross Domestic Product (GDP) Price Index from the U.S. Department of Commerce, Bureau of Economic Analysis (BEA), with 2013 as the index base.11 That is, all costs are expressed in 2013 dollars. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
Hospital stays billed to the State Children's Health Insurance Program (SCHIP) may be classified as Medicaid, Private Insurance, or Other, depending on the structure of the State program. Because most State data do not identify patients in SCHIP specifically, it is not possible to present this information separately. For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Region Region is one of the four regions defined by the U.S. Census Bureau:
Admission source or point of origin Admission source (now known as the patient's point of origin) indicates where the patient was located prior to admission to the hospital. Emergency admission indicates that the patient was admitted to the hospital through the emergency department. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health and Hospitals Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About Statistical Briefs HCUP Statistical Briefs are descriptive summary reports presenting statistics on hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, patient populations, and other topics. The reports use HCUP administrative healthcare data. About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a national (nationwide) database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
The new sampling strategy is expected to result in more precise estimates than those that resulted from the previous NIS design by reducing sampling error: for many estimates, confidence intervals under the new design are about half the length of confidence intervals under the previous design. The change in sample design for 2012 necessitates recomputation of prior years' NIS data to enable analysis of trends that uses the same definitions of discharges and hospitals. For More Information For other information on specific procedures and treatments, including red blood cell transfusions, refer to the HCUP Statistical Briefs located at http://www.hcup-us.ahrq.gov/reports/statbriefs/sb_specific.jsp. For additional HCUP statistics, visit:
For more information about HCUP, visit http://www.hcup-us.ahrq.gov/. For a detailed description of HCUP and more information on the design of the National (Nationwide) Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2015. http://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 17, 2016. Suggested Citation West KA (National Institutes of Health), Barrett ML (M.L. Barrett, Inc.), Moore BJ (Truven Health Analytics), Miller JL (National Institutes of Health), Steiner CA (Agency for Healthcare Research and Quality). Trends in Hospitalizations With a Red Blood Cell Transfusion, 2000-2013. HCUP Statistical Brief #215. December 2016. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb215-Red-Blood-Cell-Transfusions.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of Truven Health Analytics. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:David Knutson, Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on December 1, 2016. 1 U.S. Department of Health & Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. What Is a Blood Transfusion? https://www.nhlbi.nih.gov/health/health-topics/topics/bt. Accessed July 21, 2016. 2 Carson JL, Grossman BJ, Kleinman S, Tinmouth AT, Marques MB, Fung MK, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Annals of Internal Medicine. 2012;157:49-58. 3 Chung K-W, Basavaraju SV, Mu Y, van Santen KL, Haass KA, Henry R, Berger J, et al. Declining blood collection and utilization in the United States. Transfusion. 12 May 2016. doi:10.1111/trf.13644. [epub ahead of print] 4 Whitaker B, Rajbhandary S, Kleinman S, Harris A, Kamani N. Trends in United States blood collection and transfusion: results from the 2013 AABB Blood Collection, Utilization, and Patient Blood Management Survey. Transfusion. 15 June 2016. doi:10.1111/trf.13676. [epub ahead of print] 5 Pathak R, Bhatt VR, Karmacharya P, Aryal MR, Alweis R. Trends in blood-product transfusion among inpatients in the United States from 2002 to 2011: data from the Nationwide Inpatient Sample. Journal of Hospital Medicine. 2014;9:800-1. 6 Ibid. 7 Barrett M, Hickey K, Coffey R, Levit K. Population Denominator Data for Use with the HCUP Databases (Updated with 2014 Population Data). HCUP Methods Series Report #2015-07. September 1, 2015. Rockville, MD: Agency for Healthcare Research and Quality. http://www.hcup-us.ahrq.gov/reports/methods/2015-07.pdf. Accessed February 17, 2016. 8 Agency for Healthcare Research and Quality. Procedure Classes 2015. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated February 2016. http://hcup-us.ahrq.gov/toolssoftware/procedure/procedure.jsp. Accessed June 8, 2016. 9 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated October 2016. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed October 27, 2016. 10 Agency for Healthcare Research and Quality. HCUP Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). 2001-2013. Rockville, MD: Agency for Healthcare Research and Quality. Updated November 2015. http://www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed February 17, 2016. 11 U.S. Bureau of Economic Analysis. National Income and Product Account Tables, Table 1.1.4 Price Indexes for Gross Domestic Product. http://www.bea.gov/iTable/iTable.cfm?ReqID=9&step=1#reqid=9&step=1&isuri=1. |