STATISTICAL BRIEF #240 |
June 2018
(Revised October 2018)* Pamela L. Owens, Ph.D., Kevin C. Heslin, Ph.D., Kathryn R. Fingar, Ph.D., M.P.H., and Audrey J. Weiss, Ph.D. Introduction Physical health conditions and mental and/or substance use disorders (M/SUDs) are often treated, and their treatment paid for, through different mechanisms in the healthcare system.1 Increasingly it is acknowledged that physical and mental health are intertwined, that the interaction between the illnesses can worsen the course of both illnesses, and that health plan benefits for treating M/SUDs should be on par with those for medical and surgical care.2 The co-occurrence of physical health conditions and M/SUDs is high for some populations. One literature review found that the prevalence of depression and anxiety ranged from 6 percent to as high as 80 percent among patients with chronic obstructive pulmonary disease (COPD) and from 10 percent to as high as 60 percent among patients with heart failure.3 When physical health conditions and M/SUDs occur together, they may complicate diagnosis, treatment, and disease progression. Conditions often go undiagnosed among patients with co-occurring physical and mental illnesses.4 For example, COPD and heart failure may mask or mirror symptoms of depression, anxiety, and posttraumatic stress disorder, making their recognition and diagnosis less likely.5 Additionally, physical health conditions can increase risk of psychological distress, exacerbate mental disorders, and compound functional impairment.6,7 Likewise, individuals with a severe mental disorder have higher rates of chronic conditions, including hypertension and diabetes.8,9 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data on the co-occurrence of physical health conditions and M/SUDs among adult inpatient stays in 2010 and 2014. Comparisons in the 2 years are made for the prevalence of stays for M/SUDs (i.e., principal diagnosis) with a co-occurring physical health condition (i.e., secondary diagnosis) and for the prevalence of stays for physical health conditions (i.e., principal diagnosis) with a co-occurring M/SUD (i.e., secondary diagnosis). Separately, for the two types of stays—M/SUD stays with a co-occurring physical health condition and physical health stays with a co-occurring M/SUD—the following statistics are presented for 2014: (1) the distribution of stays with co-occurring conditions by type of principal diagnosis, (2) the 10 most common specific co-occurring conditions, and (3) the distribution of stays with co-occurring conditions by select patient and hospital characteristics. Differences are noted in the text only if they are 10 percent or greater. Findings Co-Occurrence of Physical Health and M/SUDs Co-occurrence of physical health conditions and M/SUDs among adult inpatient stays, 2010 versus 2014 Table 1 presents the number and percentage of adult inpatient stays involving either an M/SUD principal diagnosis with a co-occurring physical health condition, or a physical health principal diagnosis with a co-occurring M/SUD, in 2010 and 2014. |
|
| Table 1. Number and percentage of adult inpatient stays with a co-occurring physical health condition and M/SUD by principal diagnosis, 2010 and 2014 | ||||
| Principal diagnosis | Total number of stays | Stays, % | ||
|---|---|---|---|---|
| 2010 | 2014 | 2010 | 2014 | |
| M/SUD or physical health | 31,140,400 | 29,621,400 | 100.0 | 100.0 |
| Co-occurring physical condition or M/SUDa | 11,959,600 | 13,322,900 | 38.4 | 45.0 |
| No co-occurring physical condition or M/SUDa | 19,180,800 | 16,298,500 | 61.6 | 55.0 |
| M/SUD | 1,840,400 | 1,794,300 | 100.0 | 100.0 |
| Co-occurring physical health condition | 1,497,000 | 1,511,400 | 81.3 | 84.2 |
| No co-occurring physical health condition | 343,400 | 282,900 | 18.7 | 15.8 |
| Physical health | 29,300,000 | 27,827,100 | 100.0 | 100.0 |
| Co-occurring M/SUD | 10,462,600 | 11,811,500 | 35.7 | 42.4 |
| No co-occurring M/SUD | 18,837,400 | 16,015,600 | 64.3 | 57.6 |
| Abbreviation: M/SUD, mental or substance use disorder Notes: Number of stays is rounded to the nearest 100. Stays for social/administrative reasons and stays with a missing or invalid principal diagnosis were excluded from the analysis: 177,600 stays in 2010 and 130,600 stays in 2014. a Co-occurrence was defined as a principal diagnosis of either an M/SUD or a physical health condition with a secondary diagnosis of the other condition (either physical health or M/SUD). Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National (Nationwide) Inpatient Sample (NIS), 2010 and 2014 | ||||
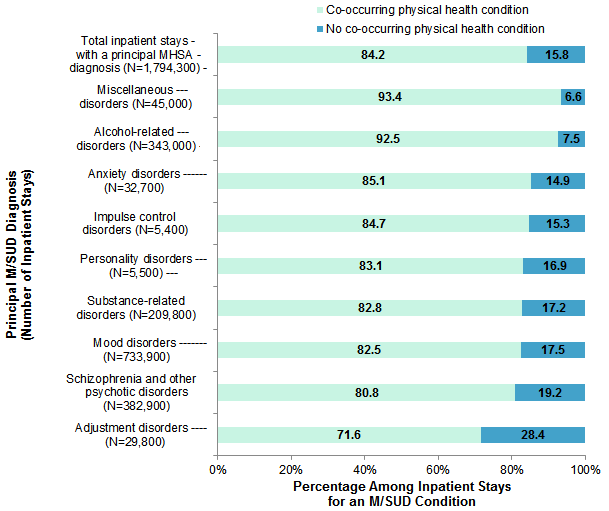
Distribution and characteristics of adult M/SUD stays with a co-occurring physical health condition, 2014 Figure 1 displays the percentage of adult inpatient stays for an M/SUD with and without a co-occurring physical health condition in 2014, by specific type of M/SUD diagnosis. |
|
Figure 1. Percentage of adult M/SUD stays with and without a co-occurring physical health condition, by type of M/SUD diagnosis, 2014
Abbreviation: M/SUD, mental or substance use disorder Bar chart that shows the percentage of adult inpatient stays with a principal M/SUD diagnosis with and without a co-occurring physical health condition by diagnosis type in 2014. Total inpatient stays with a principal M/SUD diagnosis (N=1,794,300): with co-occurring physical health condition, 84.2; with no co-occurring physical health condition, 15.8. Miscellaneous disorders (N=45,000): with co-occurring physical health condition, 93.4; with no co-occurring physical health condition, 6.6. Alcohol-related disorders (N=343,000): with co-occurring physical health condition, 92.5; with no co-occurring physical health condition, 7.5. Anxiety disorders (N=32,700): with co-occurring physical health condition, 85.1; with no co-occurring physical health condition, 14.9. Impulse control disorders (N=5,400): with co-occurring physical health condition, 84.7; with no co-occurring physical health condition, 15.3. Personality disorders (N=5,500): with co-occurring physical health condition, 83.1; with no co-occurring physical health condition, 16.9. Substance-related disorders (N=209,800): with co-occurring physical health condition, 82.8; with no co-occurring physical health condition, 17.2. Mood disorders (N=733,900): with co-occurring physical health condition, 82.5; with no co-occurring physical health condition, 17.5. Schizophrenia and other psychotic disorders (N=382,900): with co-occurring physical health condition, 80.8; with no co-occurring physical health condition, 19.2. Adjustment disorders (N=29,800): with co-occurring physical health condition, 71.6; with no co-occurring physical health condition, 28.4. |
|
| Table 2. Ten most common co-occurring physical health conditions among adult M/SUD stays (N=1,794,300), 2014 | ||
| Co-occurring physical health condition | % | |
|---|---|---|
| Essential hypertension | 30.6 | |
| Fluid and electrolyte disorders | 14.8 | |
| Esophageal disorders | 14.1 | |
| Disorders of lipid metabolism | 13.7 | |
| Diabetes without complications | 11.4 | |
| Spondylosis; intervertebral disc disorders; other back problems | 9.7 | |
| Asthma | 9.6 | |
| Deficiency and other anemia | 8.8 | |
| Thyroid disorders | 8.6 | |
| Allergic reactions | 8.3 | |
| Abbreviation: M/SUD, mental or substance use disorder Notes: Number of stays is rounded to the nearest 100. Co-occurring conditions are grouped according to the Clinical Classifications Software (CCS). Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||
|
|
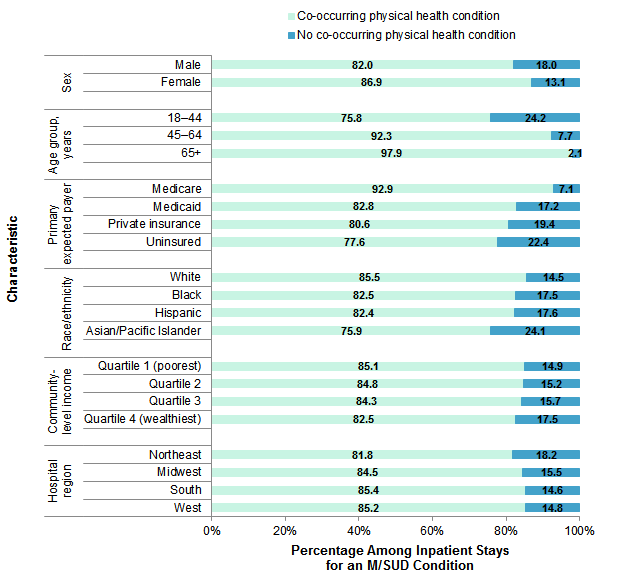
Figure 2. Percentage of adult M/SUD stays with and without a co-occurring physical health condition, by patient and hospital characteristics, 2014
Abbreviation: M/SUD, mental or substance use disorder Bar chart that shows the percentage of adult M/SUD stays with and without a co-occurring physical health condition by patient and hospital characteristics in 2014. Sex: male, 82.0 with co-occurring physical health condition and 18.0 with no co-occurring physical health condition; female, 86.9 with co-occurring physical health condition and 13.1 with no co-occurring physical health condition. Age: 18-44 years, 75.8 with co-occurring physical health condition and 24.2 with no co-occurring physical health condition; 45-64 years, 92.3 with co-occurring physical health condition and 7.7 with no co-occurring physical health condition; 65+ years, 97.9 with co-occurring physical health condition and 2.1 with no co-occurring physical health condition. Primary expected payer: Medicare, 92.9 with co-occurring physical health condition and 7.1 with no co-occurring physical health condition; Medicaid, 82.8 with co-occurring physical health condition and 17.2 with no co-occurring physical health condition; private insurance, 80.6 with co-occurring physical health condition and 19.4 with no co-occurring physical health condition; uninsured, 77.6 with co-occurring physical health condition and 22.4 with no co-occurring physical health condition. Race/ethnicity: White, 85.5 with co-occurring physical health condition and 14.5 with no co-occurring physical health condition; Black, 82.5 with co-occurring physical health condition and 17.5 with no co-occurring physical health condition; Hispanic, 82.4 with co-occurring physical health condition and 17.6 with no co-occurring physical health condition; Asian/Pacific Islander, 75.9 with co-occurring physical health condition and 24.1 with no co-occurring physical health condition. Community-level income: Quartile 1 (lowest), 85.1 with co-occurring physical health condition and 14.9 with no co-occurring physical health condition; Quartile 2, 84.8 with co-occurring physical health condition and 15.2 with no co-occurring physical health condition; Quartile 3, 84.3 with co-occurring physical health condition and 15.7 with no co-occurring physical health condition; Quartile 4 (wealthiest), 82.5 with co-occurring physical health condition and 17.5 with no co-occurring physical health condition. Hospital region: Northeast, 81.8 with co-occurring physical health condition and 18.2 with no co-occurring physical health condition; Midwest, 84.5 with co-occurring physical health condition and 15.5 with no co-occurring physical health condition; South, 85.4 with co-occurring physical health condition and 14.6 with no co-occurring physical health condition; West, 85.2 with co-occurring physical health condition and 14.8 with no co-occurring physical health condition.
|
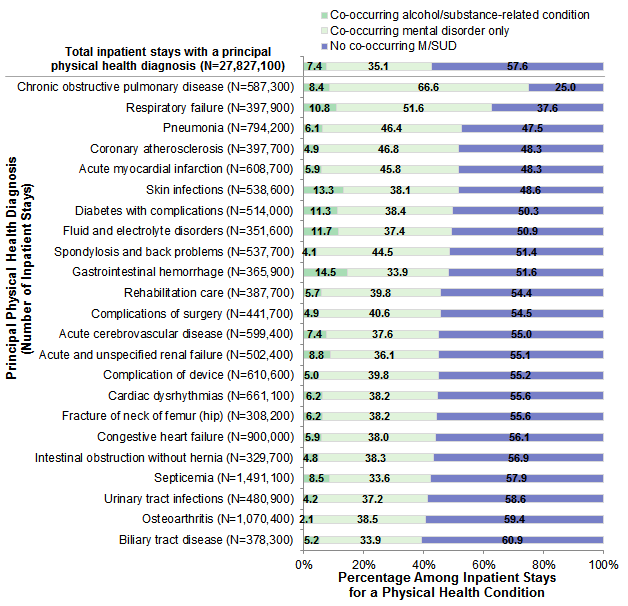
Distribution and characteristics of adult physical health stays with a co-occurring M/SUD, 2014 Figure 3 displays the percentage of adult inpatient stays for a physical health condition with and without a co-occurring M/SUD in 2014, by specific type of physical health condition. Stays with a co-occurring M/SUD were subdivided into those with a co-occurring alcohol/substance-related condition (with or without a co-occurring mental disorder) and those with a co-occurring mental disorder only (i.e., without a co-occurring alcohol/substance-related condition). |
|
Figure 3. Percentage of adult physical health stays with and without a co-occurring M/SUD, by type of physical health diagnosis, 2014
Abbreviation: M/SUD, mental or substance use disorder Bar chart that shows the percentage of principal adult physical health stays with and without a co-occurring M/SUD by physical health diagnosis type in 2014. Total (N=27,827,100): 7.4 with co-occurring alcohol/substance-related condition, 35.1 with co-occurring mental disorder only, 57.6 with no co-occurring M/SUD. Chronic obstructive pulmonary disease (N=587,300): 8.4 with co-occurring alcohol/substance-related condition, 66.6 with co-occurring mental disorder only, 25.0 with no co-occurring M/SUD. Respiratory failure (N=397,900): 10.8 with co-occurring alcohol/substance-related condition, 51.6 with co-occurring mental disorder only, 37.6 with no co-occurring M/SUD. Pneumonia (N=794,200): 6.1 with co-occurring alcohol/substance-related condition, 46.4 with co-occurring mental disorder only, 47.5 with no co-occurring M/SUD. Coronary atherosclerosis (N=397,700): 4.9 with co-occurring alcohol/substance-related condition, 46.8 with co-occurring mental disorder only, 48.3 with no co-occurring M/SUD. Acute myocardial infarction (N=608,700): 5.9 with co-occurring alcohol/substance-related condition, 45.8 with co-occurring mental disorder only, 48.3 with no co-occurring M/SUD. Skin infections (N=538,600): 13.3 with co-occurring alcohol/substance-related condition, 38.1 with co-occurring mental disorder only, 48.6 with no co-occurring M/SUD. Diabetes with complications (N=514,000): 11.3 with co-occurring alcohol/substance-related condition, 38.4 with co-occurring mental disorder only, 50.3 with no co-occurring M/SUD. Fluid and electrolyte disorders (N=351,600): 11.7 with co-occurring alcohol/substance-related condition, 37.4 with co-occurring mental disorder only, 50.9 with no co-occurring M/SUD. Spondylosis and back problems (N=537,700): 4.1 with co-occurring alcohol/substance-related condition, 44.5 with co-occurring mental disorder only, 51.4 with no co-occurring M/SUD. Gastrointestinal hemorrhage (N=365,900): 14.5 with co-occurring alcohol/substance-related condition, 33.9 with co-occurring mental disorder only, 51.6 with no co-occurring M/SUD. Rehabilitation care (N=387,700): 5.7 with co-occurring alcohol/substance-related condition, 39.8 with co-occurring mental disorder only, 54.4 with no co-occurring M/SUD. Complications of surgery (N=441,700): 4.9 with co-occurring alcohol/substance-related condition, 40.6 with co-occurring mental disorder only, 54.5 with no co-occurring M/SUD. Acute cerebrovascular disease (N=599,400): 7.4 with co-occurring alcohol/substance-related condition, 37.6 with co-occurring mental disorder only, 55.0 with no co-occurring M/SUD. Acute and unspecified renal failure (N=502,400): 8.8 with co-occurring alcohol/substance-related condition, 36.1 with co-occurring mental disorder only, 55.1 with no co-occurring M/SUD. Complication of device (N=610,600): 5.0 with co-occurring alcohol/substance-related condition, 39.8 with co-occurring mental disorder only, 55.2 with no co-occurring M/SUD. Cardiac dysrhythmias (N=661,100): 6.2 with co-occurring alcohol/substance-related condition, 38.2 with co-occurring mental disorder only, 55.6 with no co-occurring M/SUD. Fracture of neck of femur (hip) (N=308,200): 6.2 with co-occurring alcohol/substance-related condition, 38.2 with co-occurring mental disorder only, 55.6 with no co-occurring M/SUD. Congestive heart failure (N=900,000): 5.9 with co-occurring alcohol/substance-related condition, 38.0 with co-occurring mental disorder only, 56.1 with no co-occurring M/SUD. Intestinal obstruction without hernia (N=329,700): 4.8 with co-occurring alcohol/substance-related condition, 38.3 with co-occurring mental disorder only, 56.9 with no co-occurring M/SUD. Septicemia (N=1,491,100): 8.5 with co-occurring alcohol/substance-related condition, 33.6 with co-occurring mental disorder only, 57.9 with no co-occurring M/SUD. Urinary tract infections (N=480,900): 4.2 with co-occurring alcohol/substance-related condition, 37.2 with co-occurring mental disorder only, 58.6 with no co-occurring M/SUD. Osteoarthritis (N=1,070,400): 2.1 with co-occurring alcohol/substance-related condition, 38.5 with co-occurring mental disorder only, 59.4 with no co-occurring M/SUD. Biliary tract disease (N=378,300): 5.2 with co-occurring alcohol/substance-related condition, 33.9 with co-occurring mental disorder only, 60.9 with no co-occurring M/SUD.
|
|
| Table 3. Ten most common co-occurring M/SUDs among adult physical health stays (N=27,827,100), 2014 | ||
| Co-occurring M/SUD | N | % |
|---|---|---|
| Screening and history of mental health and substance abuse codes | 7,449,100 | 26.8 |
| Mood disorders | 3,937,700 | 14.2 |
| Anxiety disorders | 2,866,700 | 10.3 |
| Alcohol-related disorders | 1,160,600 | 4.2 |
| Substance-related disorders | 1,114,100 | 4.0 |
| Schizophrenia and other psychotic disorders | 439,300 | 1.6 |
| Miscellaneous disorders | 301,000 | 1.1 |
| Attention-deficit, conduct, and disruptive behavior disorders | 124,300 | 0.4 |
| Adjustment disorders | 91,100 | 0.3 |
| Suicide, intentional self-inflicted injury | 74,800 | 0.3 |
| Abbreviation: M/SUD, mental or substance use disorder Notes: Number of stays is rounded to the nearest 100. Co-occurring conditions are grouped according to the Clinical Classifications Software (CCS). Miscellaneous disorders include eating, sexual, and sleep-related disorders as well as other unspecified behavioral disorders. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2014 | ||
|
|
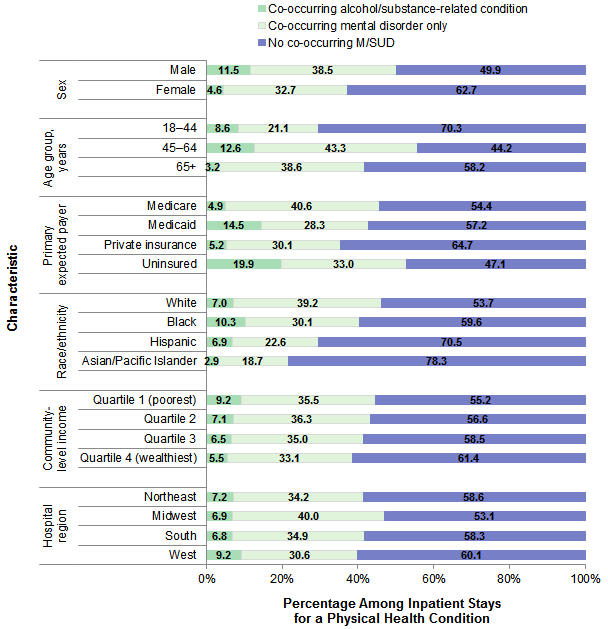
Figure 4. Percentage of adult physical health stays with and without a co-occurring M/SUD, by patient and hospital characteristics, 2014
Abbreviation: M/SUD, mental or substance use disorder Bar chart that shows the percentage of adult physical health stays with and without a co-occurring M/SUD by patient and hospital characteristics in 2014. Sex: male, 11.5 with co-occurring alcohol/substance-related condition, 38.5 with co-occurring mental disorder only, and 49.9 with no co-occurring physical health condition; female, 4.6 with co-occurring alcohol/substance-related condition, 32.7 with no co-occurring physical health condition, and 62.7 with no co-occurring M/SUD. Age: 18-44 years, 8.6 with co-occurring alcohol/substance-related condition, 21.1 with co-occurring mental disorder only, and 70.3 with no co-occurring M/SUD; 45-64 years, 12.6 with co-occurring alcohol/substance-related condition, 43.3 with co-occurring mental disorder only, and 44.2 with no co-occurring M/SUD; 65+ years, 3.2 with co-occurring alcohol/substance-related condition, 38.6 with co-occurring mental disorder only, and 58.2 with no co-occurring M/SUD. Primary expected payer: Medicare, 4.9 with co-occurring alcohol/substance-related condition, 40.6 with co-occurring mental disorder only, and 54.4 with no co-occurring M/SUD; Medicaid, 14.5 with co-occurring alcohol/substance-related condition, 28.3 with co-occurring mental disorder only, and 57.2 with no co-occurring M/SUD; private insurance, 5.2 with co-occurring alcohol/substance-related condition, 30.1 with co-occurring mental disorder only, and 64.7 with no co-occurring M/SUD; uninsured, 19.9 with co-occurring alcohol/substance-related condition, 33.0 with co-occurring mental disorder only, and 47.1 with no co-occurring M/SUD. Race/ethnicity: White, 7.0 with co-occurring alcohol/substance-related condition, 39.2 with co-occurring mental disorder only, and 53.7 with no co-occurring M/SUD; Black, 10.3 with co-occurring alcohol/substance-related condition, 30.1 with co-occurring mental disorder only, and 59.6 with no co-occurring M/SUD; Hispanic, 6.9 with co-occurring alcohol/substance-related condition, 22.6 with co-occurring mental disorder only, and 70.5 with no co-occurring M/SUD; Asian/Pacific Islander, 2.9 with co-occurring alcohol/substance-related condition, 18.7 with co-occurring mental disorder only, and 78.3 with no co-occurring M/SUD. Community-level income: Quartile 1 (lowest), 9.2 with co-occurring alcohol/substance-related condition, 35.5 with co-occurring mental disorder only, and 55.2 with no co-occurring M/SUD; Quartile 2, 7.1 with co-occurring alcohol/substance-related condition, 36.3 with co-occurring mental disorder only, and 56.6 with no co-occurring M/SUD; Quartile 3, 6.5 with co-occurring alcohol/substance-related condition, 35.0 with co-occurring mental disorder only, and 58.5 with no co-occurring M/SUD; Quartile 4 (wealthiest), 5.5 with co-occurring alcohol/substance-related condition, 33.1 with co-occurring mental disorder only, and 61.4 with no co-occurring M/SUD. Hospital region: Northeast, 7.2 with co-occurring alcohol/substance-related condition, 34.2 with co-occurring mental disorder only, and 58.6 with no co-occurring M/SUD; Midwest, 6.9 with co-occurring alcohol/substance-related condition, 40.0 with co-occurring mental disorder only, and 53.1 with no co-occurring M/SUD; South, 6.8 with co-occurring alcohol/substance-related condition, 34.9 with co-occurring mental disorder only, and 58.3 with no co-occurring M/SUD; West, 9.2 with co-occurring alcohol/substance-related condition, 30.6 with co-occurring mental disorder only, and 60.1 with no co-occurring M/SUD.
|
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from the HCUP 2014 National Inpatient Sample (NIS). Historical data were drawn from the 2010 Nationwide Inpatient Sample (NIS). Supplemental sources included population denominator data for use with HCUP databases, derived from information available from the U.S. Census Bureau.10 Definitions Diagnoses, ICD-9-CM, and Clinical Classifications Software (CCS) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses. There are approximately 14,000 ICD-9-CM diagnosis codes. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.11 This clinical grouper makes it easier to quickly understand patterns of diagnoses. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. Case definition The CCS categories defining mental or substance use disorder (M/SUD) and physical health diagnoses are shown in Table 4. CCS categories classified as neither M/SUD nor physical health are not often listed as a principal diagnosis and include codes such as those for social/administrative issues (e.g., homelessness) that may provide context for a stay related to an M/SUD or physical health condition. Inpatient stays with a principal CCS category classified as neither M/SUD nor physical health were excluded from the analysis, as were stays with a missing or invalid principal diagnosis; in total, 177,600 stays were excluded in 2010 and 130,600 stays were excluded in 2014. |
| Table 4. CCS categories defining M/SUD and physical health conditions | ||
| CCS number | CCS description | Categorization |
|---|---|---|
| 650 | Adjustment disorders | M/SUD |
| 651 | Anxiety disorders | M/SUD |
| 652 | Attention-deficit, conduct, and disruptive behavior disorders | M/SUD |
| 655 | Disorders usually diagnosed in infancy, childhood, or adolescence | M/SUD |
| 656 | Impulse control disorders, not elsewhere classifiable | M/SUD |
| 657 | Mood disorders | M/SUD |
| 658 | Personality disorders | M/SUD |
| 659 | Schizophrenia and other psychotic disorders | M/SUD |
| 660 | Alcohol-related disorders | M/SUD |
| 661 | Substance-related disorders | M/SUD |
| 662 | Suicide and intentional self-inflicted injury | M/SUD |
| 663 | Screening and history of mental health and substance abuse codes | M/SUD |
| 670 | Miscellaneous mental health disorders | M/SUD |
| 653 | Delirium, dementia, and amnestic and other cognitive disorders | Physical |
| 654 | Developmental disorders | Physical |
| 255 | Administrative/social admission | Neither |
| 256 | Medical examination/evaluation | Neither |
| 257 | Other aftercare | Neither |
| 258 | Other screening for suspected conditions (not mental disorders or infectious disease) | Neither |
| 259 | Residual codes; unclassified | Neither |
| 1-254, 2601-2621 | See CCS documentationa | Physical |
| Abbreviations: CCS, Clinical Classifications Software, M/SUD, mental or substance use disorder a Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated March 2017. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed January 18, 2018. | ||
Co-occurrence was defined as a principal CCS diagnosis of either an M/SUD or a physical health condition with a secondary CCS diagnosis of the other condition (either physical health or M/SUD). Thus, there were two types of stays involving the co-occurrence of M/SUD and physical health conditions: (1) an M/SUD principal diagnosis with a secondary diagnosis of a physical health condition and (2) a physical health condition principal diagnosis with a secondary diagnosis of an M/SUD condition.
For Figures 3 and 4, physical health stays with a co-occurring M/SUD condition were subdivided into two categories:
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Community-level income Community-level income is based on the median household income of the patient's ZIP Code of residence. Quartiles are defined so that the total U.S. population is evenly distributed. Cut-offs for the quartiles are determined annually using ZIP Code demographic data obtained from Claritas, a vendor that adds value to data from the U.S. Census Bureau.12 The value ranges for the income quartiles vary by year. The income quartile is missing for patients who are homeless or foreign. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Region Region is one of the four regions defined by the U.S. Census Bureau:
Data on Hispanic ethnicity are collected differently among the States and also can differ from the census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other (including mixed race)) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, and Asian/Pacific Islander. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
For More Information For other information on mental health and substance abuse, including opioids, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_mhsa.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National (Nationwide) Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated February 2018. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 12, 2018. Suggested Citation Owens PL (AHRQ), Heslin KC (AHRQ), Fingar KR (IBM Watson Health), Weiss AJ (IBM Watson Health). Co-occurrence of Physical Health Conditions and Mental Health and Substance Use Conditions Among Adult Inpatient Stays, 2010 Versus 2014. HCUP Statistical Brief #240. June 2018. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb240-Co-occurring-Physical-Mental-Substance-Conditions-Hospital-Stays.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Virginia Mackay-Smith, Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on June 26, 2018. The revised version of this Statistical Brief was posted online on October 17, 2018. * This Statistical Brief was revised to include information on how many inpatient stays with a principal physical health diagnosis had a co-occurring M/SUD diagnosis related to tobacco use. This information is included on page 9. 1 Horvitz-Lennon M, Kilbourne AM, Pincus HA. From silos to bridges: meeting the general healthcare needs of adults with severe mental illnesses. Health Affairs (Millwood). 2006;25(3):659-69. 2 Substance Abuse and Mental Health Services Administration. Implementation of the Mental Health Parity and Addiction Equity Act (MHPAEA). January 24, 2017. www.samhsa.gov/health-financing/implementation-mental-health-parity-addiction-equity-act. Accessed September 21, 2017. 3 Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. International Journal of Geriatric Psychiatry. 2010;25(12):1209-21. 4 Horvitz-Lennon et al., 2006. Op. cit. 5 Ratcliff CG, Barrera TL, Petersen NJ, Sansgiry S, Kauth MR, Kunik ME, et al. Recognition of anxiety, depression, and PTSD in patients with COPD and CHF: who gets missed? General Hospital Psychiatry. 2017;47:61-7. 6 Horvitz-Lennon M, Kilbourne AM, Pincus HA. From silos to bridges: meeting the general healthcare needs of adults with severe mental illnesses. Health Affairs (Millwood). 2006;25(3):659-69. 7 Whooley MD, de Jonge P, Vittinghoff E, Otte C, Moos R, Carney RM, et al. Depressive symptoms, health behaviors, and risk of cardiovascular events in patients with coronary heart disease. JAMA. 2008;300(20):2379-88. 8 Horvitz-Lennon et al., 2006. Op. cit. 9 Sokal J, Messias E, Dickerson FB, Kreyenbuhl J, Brown CH, Goldberg RW, et al. Comorbidity of medical illnesses among adults with serious mental illness who are receiving community psychiatric services. Journal of Nervous and Mental Disease. 2004;192(6):421-7. 10 Barrett M, Coffey R, Levit K. Population Denominator Data for Use with the HCUP Databases (Updated with 2016 Population Data). HCUP Methods Series Report #2016-04. October 17, 2017. U.S. Agency for Healthcare Research and Quality. www.hcup-us.ahrq.gov/reports/methods/2017-04.pdf. Accessed January 18, 2018. 11 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated March 2017. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed January 18, 2018. 12 Claritas. Claritas Demographic Profile by ZIP Code. https://claritas360.claritas.com/mybestsegments/. |