STATISTICAL BRIEF #245 |
November 2018
Kathryn R. Fingar, Ph.D., M.P.H., Halcyon Skinner, Ph.D., M.P.H., Jayne Johann, M.B.A., Natalia Coenen, M.P.H., William J. Freeman, Dr.P.H., M.P.H., and Kevin C. Heslin, Ph.D. Introduction Substance use disorders contribute to the burden of disease at a higher rate in the United States than in other developed countries.1 Individuals with a substance use disorder are at greater risk of major medical conditions and adverse outcomes such as cardiovascular disease and cancer, mortality, and mental health problems, including suicidal thoughts and behaviors.2,3 On a societal level, substance use disorders are associated with greater healthcare utilization and costs, crime, and lost work productivity.4 Reducing the prevalence of these disorders is critical for fostering the physical and mental health, safety, and well-being of individuals, families, and communities across the United States.5 Alcohol is the most common type of substance abused, which may be in part because it is easier to access than other substances.6 In 2013, 17.3 million Americans were dependent on or had problems related to their use of alcohol, down from 18.1 million in 2002.7 Marijuana was the next most common type of substance involving abuse or dependence (4.2 million individuals), followed by prescription pain relievers (1.8 million individuals), cocaine (855,000 individuals), heroin (517,000 individuals), and stimulants other than cocaine (469,000 individuals).8 Use of multiple types of substances also is common and increases risk of hospitalization, overdose, and death.9 One in nine people with a substance use disorder have both alcohol and drug dependence.10 The proportion of the U.S. population with alcohol dependence decreased by 14 percent between 2002 and 2013 (from 7.7 percent to 6.6 percent of the population).11 However, other data show that the rate of alcohol-related inpatient stays increased by 33 percent between 2013 and 2014 alone (from 81.4 to 108.0 stays per 100,000 population).12 The opioid crisis—which has resulted from the abuse of both prescription and illegal drugs, including heroin—also has grown. Prescriptions for pain relievers did in fact decrease from 2012 through 2016, from 81.3 to 66.5 prescriptions per 100 persons—the lowest rate in over 10 years.13 Nevertheless, opioid-related emergency department visits have continued to rise (by 99 percent between 2005 and 2014), as have opioid-related hospitalizations (by 64 percent between 2005 and 2014), and deaths (by 180 percent between 2002 and 2015).14,15 An estimated 22.7 million Americans need treatment for a problem related to alcohol or drugs, but only a small fraction (<1 percent) receive it.16 Furthermore, access to treatment varies widely across the United States.17,18 Although substance use can be addressed effectively in ambulatory care and other community settings, hospitalization remains a key component of the continuum of care for individuals with a substance use disorder. A better understanding of geographic variation in types of substance-related hospitalizations across the country may inform State and local efforts to increase access to substance use disorder treatment. This Healthcare Cost and Utilization Project (HCUP) Statistical Brief examines State- and county-level variation in substance-related inpatient stays in 31 States that, at the time this Statistical Brief was written, released data through the Community-Level Statistics path of HCUPnet, an online query tool for county- and substate region-level statistics.19 Aggregate data from 2013 through the third quarter of 2015 are presented. The fourth quarter of 2015 is excluded because of the transition of the International Classification of Diseases coding system from the 9th to the 10th revision.20 First, State-level rates of inpatient stays involving common types of substances are shown. Second, county-level rates of stays involving the four most common types of substances (alcohol, opioids, cannabis, and stimulants) are examined. Finally, the cost of substance-related stays overall and for these four substances is presented for each State. If an inpatient stay involved multiple substances, the stay was counted in each substance type. Data are suppressed for counties if they are based on a small number of inpatient stays or hospitals, if they are statistically unstable, or if there was incomplete reporting. Thus, in this Statistical Brief, the highest and lowest rates of substance-related stays are described only among counties with unsuppressed data. All differences noted in the text are 10 percent or greater. Readers should note that the substance definitions used in this Statistical Brief were developed for the Community-Level Statistics path of HCUPnet.21 The definitions may differ from those in other Statistical Briefs. In particular, the opioid definition used here includes opioid dependence/abuse in remission and neonatal abstinence syndrome and does not include opioid substances causing adverse effects in therapeutic use. As a result, rates of substance-related inpatient stays may differ somewhat from similar rates reported elsewhere (e.g., opioid statistics available in HCUP Fast Stats, statistics based on the Clinical Classification Software category for substance-related disorders). Findings State-level rates of inpatient stays involving common types of substances, 2013-2015 Table 1 presents the leading types of substances involved in inpatient stays within 31 States and the nation overall. The State-level rate of stays per 100,000 population is presented for all substances combined, including the most common types of substances shown, as well as other types of substances that are not shown, such as sedatives. For each of the three most common types of substances, the State-level rate and share of stays, as a percentage of total stays for all substance types, are shown. Data are sorted in descending order by the rate of total stays for all types of substances combined. An inpatient stay may be counted under multiple categories if it involved more than one type of substance. |
|
| Table 1. State-level rates of common types of substance-related inpatient stays, 2013-2015 | ||||||||||
| State | Ratea of stays for all substances | Most common substance type | Second most common substance type | Third most common substance type | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type | Ratea | % | Type | Ratea | % | Type | Ratea | % | ||
| United States | 1,064 | Alcohol | 588 | 55.3 | Opioid | 217 | 20.4 | Cannabis | 193 | 18.1 |
| Rhode Island | 1,503 | Alcohol | 894 | 59.5 | Opioid | 336 | 22.3 | Cannabis | 250 | 16.6 |
| Massachusetts | 1,387 | Alcohol | 839 | 60.5 | Opioid | 373 | 26.9 | Cannabis | 190 | 13.7 |
| West Virginia | 1,344 | Alcohol | 677 | 50.4 | Opioid | 401 | 29.9 | Otherb | 250 | 18.6 |
| Maryland | 1,329 | Alcohol | 723 | 54.4 | Opioid | 411 | 30.9 | Cannabis | 269 | 20.3 |
| Florida | 1,289 | Alcohol | 715 | 55.5 | Opioid | 218 | 16.9 | Cannabis | 217 | 16.9 |
| Michigan | 1,217 | Alcohol | 677 | 55.6 | Cannabis | 298 | 24.5 | Opioid | 236 | 19.4 |
| Tennessee | 1,204 | Alcohol | 574 | 47.7 | Opioid | 341 | 28.3 | Other b | 222 | 18.4 |
| Minnesota | 1,188 | Alcohol | 734 | 61.8 | Cannabis | 230 | 19.3 | Opioid | 214 | 18.0 |
| Kentucky | 1,173 | Alcohol | 559 | 47.6 | Opioid | 312 | 26.6 | Otherb | 239 | 20.3 |
| Illinois | 1,162 | Alcohol | 640 | 55.1 | Opioid | 267 | 23.0 | Cannabis | 234 | 20.2 |
| New Mexico | 1,139 | Alcohol | 674 | 59.2 | Opioid | 223 | 19.6 | Cannabis | 182 | 16.0 |
| Pennsylvania | 1,129 | Alcohol | 617 | 54.6 | Opioid | 280 | 24.7 | Cannabis | 163 | 14.5 |
| Oregon | 1,106 | Alcohol | 573 | 51.8 | Opioid | 270 | 24.4 | Stimulant | 201 | 18.1 |
| Arizona | 1,098 | Alcohol | 564 | 51.3 | Opioid | 223 | 20.3 | Stimulant | 184 | 16.7 |
| North Carolina | 1,087 | Alcohol | 574 | 52.8 | Cannabis | 227 | 20.9 | Opioid | 203 | 18.7 |
| New Jersey | 1,077 | Alcohol | 583 | 54.1 | Opioid | 294 | 27.3 | Cannabis | 173 | 16.1 |
| Wisconsin | 1,033 | Alcohol | 665 | 64.4 | Opioid | 173 | 16.7 | Cannabis | 153 | 14.8 |
| Washington | 1,021 | Alcohol | 495 | 48.5 | Opioid | 300 | 29.4 | Cannabis | 185 | 18.1 |
| Indiana | 976 | Alcohol | 536 | 55.0 | Opioid | 192 | 19.6 | Cannabis | 179 | 18.4 |
| Oklahoma | 970 | Alcohol | 485 | 49.7 | Other b | 185 | 19.1 | Cannabis | 150 | 15.5 |
| California | 945 | Alcohol | 503 | 53.2 | Stimulant | 221 | 23.4 | Cannabis | 169 | 17.9 |
| North Dakota | 945 | Alcohol | 634 | 67.2 | Cannabis | 166 | 17.6 | Opioid | 147 | 15.6 |
| South Carolina | 931 | Alcohol | 553 | 59.4 | Cannabis | 172 | 18.4 | Stimulant | 144 | 15.5 |
| Nevada | 923 | Alcohol | 501 | 54.2 | Opioid | 168 | 18.2 | Stimulant | 153 | 16.5 |
| Wyoming | 912 | Alcohol | 629 | 69.0 | Cannabis | 132 | 14.5 | Opioid | 101 | 11.0 |
| Arkansas | 881 | Alcohol | 432 | 49.0 | Cannabis | 161 | 18.3 | Stimulant | 147 | 16.6 |
| Louisiana | 867 | Alcohol | 425 | 49.0 | Cannabis | 167 | 19.2 | Opioid | 151 | 17.5 |
| Hawaii | 863 | Alcohol | 401 | 46.5 | Stimulant | 280 | 32.5 | Cannabis | 196 | 22.7 |
| Texas | 690 | Alcohol | 396 | 57.4 | Stimulant | 124 | 18.0 | Cannabis | 119 | 17.3 |
| Utah | 624 | Alcohol | 282 | 45.1 | Opioid | 187 | 29.9 | Stimulant | 119 | 19.1 |
| Iowa | 624 | Alcohol | 418 | 67.0 | Cannabis | 74 | 11.8 | Otherb | 63 | 10.1 |
|
a The rate of inpatient stays per 100,000 population was calculated annually and then averaged across the 3 years (2013-2015), weighted by the population total in each year. State-level rates are based on data from all counties, including those with suppressed county-level data in subsequent figures. b Other drug abuse includes such things as combinations of or unspecified drug dependence, drug dependence complicating pregnancy, antidepressant abuse, and poisoning by common cold medicines. A full definition is provided in Table 3 starting on page 23. Note: Inpatient stays may involve more than one type of substance. Thus, substance-specific rates may sum to more than the rate for all substances combined. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), 2013-2015 National Inpatient Sample (NIS) and 2013-2015 State Inpatient Databases (SID) for 31 States, which, at the time this Statistical Brief was written, released data through the Community-Level Statistics path on HCUPnet, an online query tool. | ||||||||||
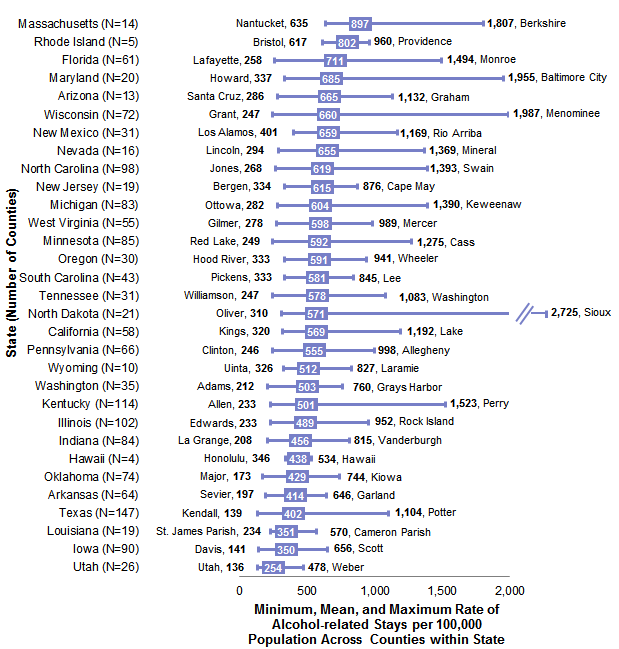
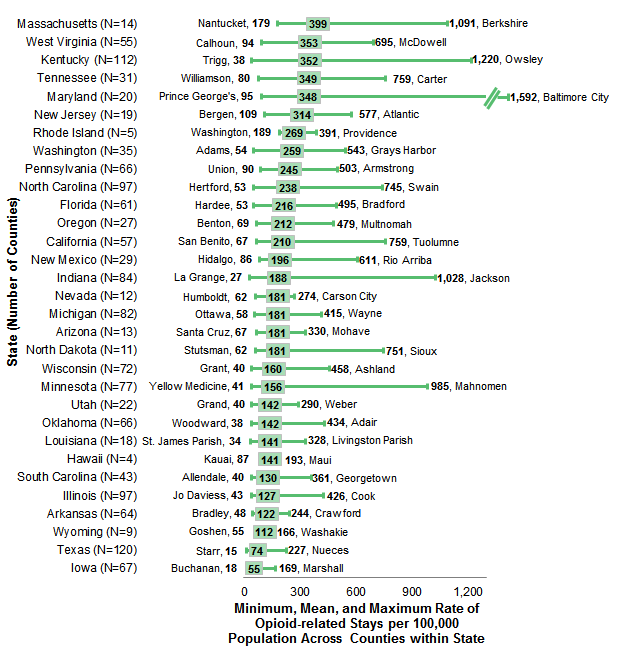
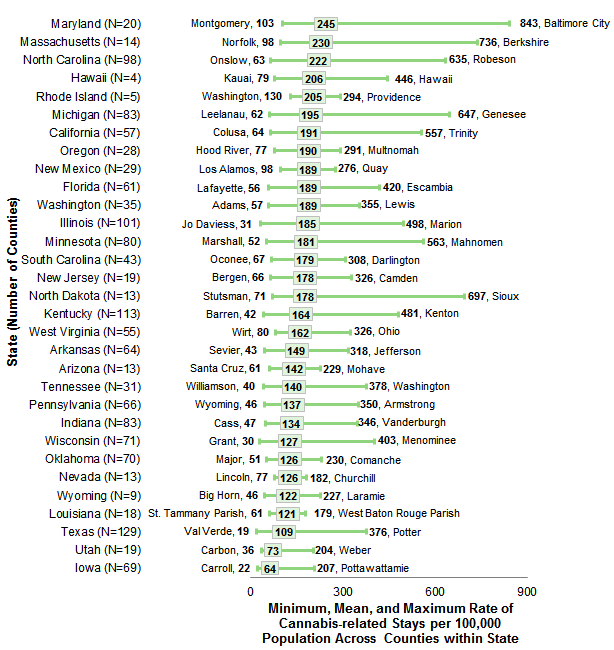
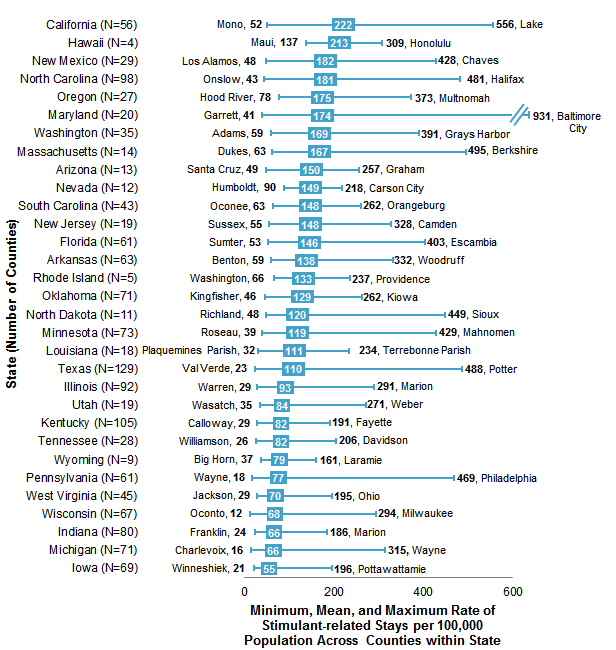
Alcohol was the most common type of substance among inpatient stays overall and in each of the 31 States. At the national level, there were 588 alcohol-related stays per 100,000 population and alcohol was involved in 55.3 percent of all substance-related stays. At the State level, the rate of alcohol-related stays ranged from 282 per 100,000 population in Utah to 894 per 100,000 population in Rhode Island. Figures 1 through 4 present characteristics of the distributions of county-level rates of inpatient stays involving the four most common types of substances: alcohol, opioids, cannabis, and stimulants. The figures display the minimum, mean, and maximum rate (per 100,000 population) across counties within the 31 States included in this Brief. The county name is listed alongside the minimum and maximum values. The States are ordered according to the mean county-level rate. Note that the means of county-level rates in Figures 1-4 (averaged across all counties in each State)22 may differ from the State-level rates presented in Table 1. |
|
Figure 1. County-level variation in rates of alcohol-related inpatient stays, by State, 2013-2015
Abbreviation: N, number of counties in the State with unsuppressed data Cluster bar chart that shows rate of alcohol-related inpatient stays per 100,000 population in the county with the highest and lowest rate and the mean rate by State from 2013 to 2015. Data are provided in Supplemental Table 1.
|
|
|
Figure 2. County-level variation in rates of opioid-related inpatient stays, by State, 2013-2015
Abbreviation: N, number of counties in the State with unsuppressed data Cluster bar chart that shows rate of opioid-related inpatient stays per 100,000 population in the county with the highest and lowest rate and the mean rate by State from 2013 to 2015. Data are provided in Supplemental Table 2.
|
|
|
Figure 3. County-level variation of rates of cannabis-related inpatient stays, by State, 2013-2015
Abbreviation: N, number of counties in the State with unsuppressed data Cluster bar chart that shows rate of cannabis-related inpatient stays per 100,000 population in the county with the highest and lowest rate and the mean rate by State from 2013 to 2015. Data are provided in Supplemental Table 3.
|
|
|
Figure 4. County-level variation in rates of stimulant-related inpatient stays, by State, 2013-2015
Abbreviation: N, number of counties in the State with unsuppressed data Cluster bar chart that shows rate of stimulant-related inpatient stays per 100,000 population in the county with the highest and lowest rate and the mean rate by State from 2013 to 2015. Data are provided in Supplemental Table 4.
|
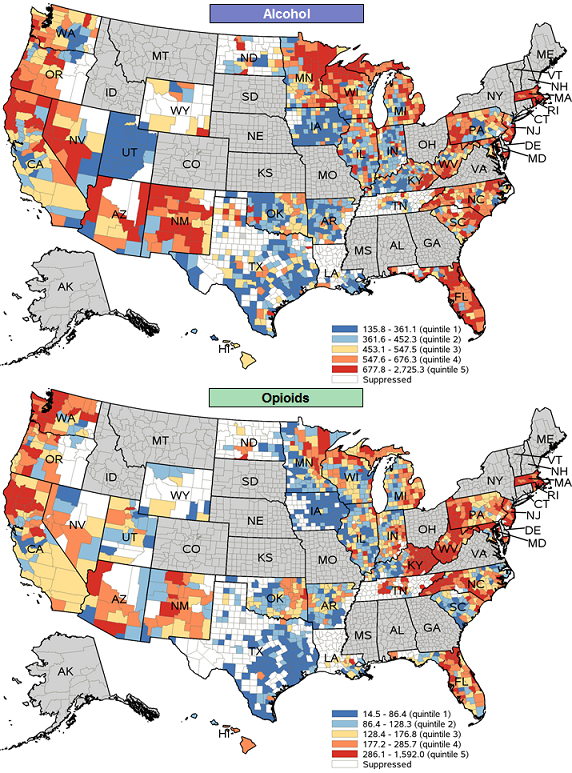
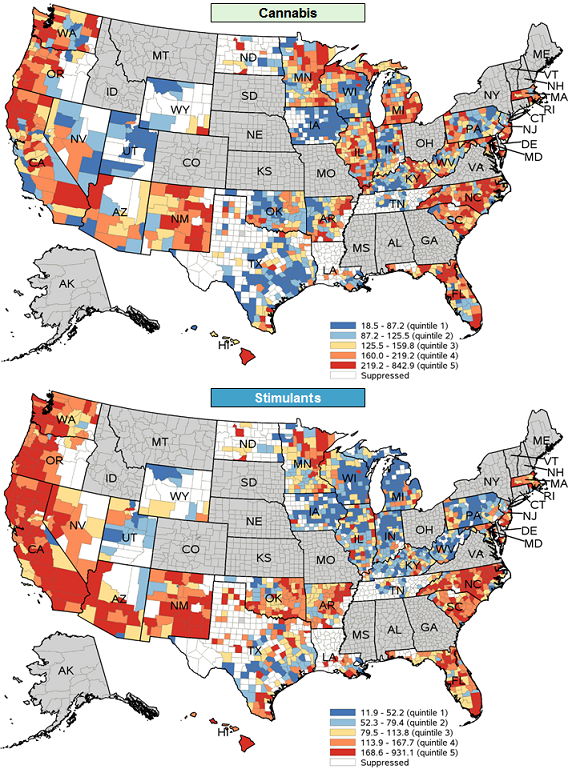
Figures 5 and 6 display maps of county-level rates of alcohol-, opioid-, cannabis-, and stimulant-related inpatient stays in 2013-2015 for the 31 States included in this Brief. Rates were categorized into quintiles after ranking all counties in the 31 States with data that were not suppressed. Counties with rates in the highest quintile (top 20 percent) were considered hot spots. |
|
Figure 5. County-level rates of alcohol- and opioid-related inpatient stays per 100,000 population, 2013-2015
|
|
|
Figure 6. County-level rates of cannabis- and stimulant-related inpatient stays per 100,000 population, 2013-2015
|
|
|
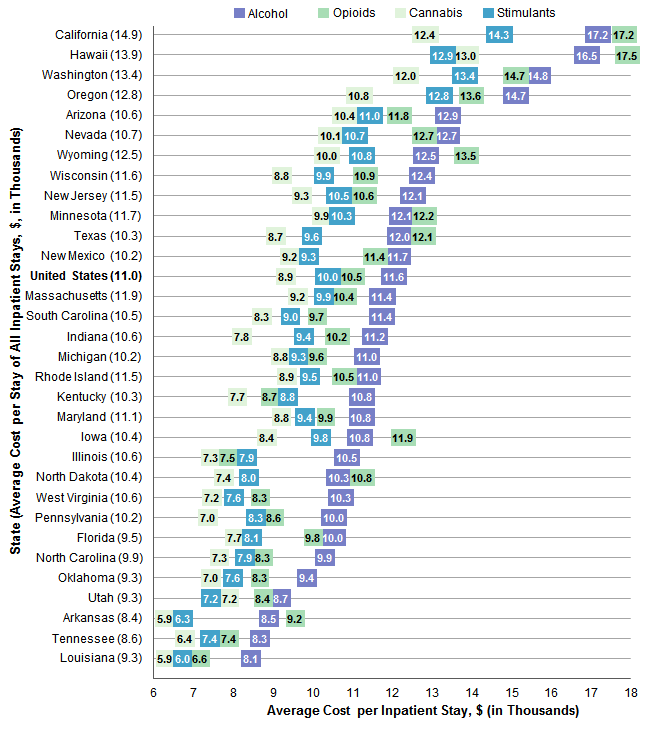
Figure 7. Average cost per type of substance-related inpatient stay, by State, 2013-2015
Note: Average cost per stay was calculated annually and then averaged across the 3 years (2013-2015), weighted by the population total. Clustered bar chart that shows average cost in thousands of dollars of substance-related inpatient stays for all stays and for alcohol, opioids, cannabis, and stimulants for 2013 to 2015. Data are provided in Supplemental Table 5.
|
| Table 2. Per capita costs of inpatient stays involving substance use and the prevalence of hot spots for substance-related stays, by State, 2013-2015 | |||||||||
| State | Per capita cost, $a | Counties in the State that were hot spotsb for types of substance-related stays, % | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All substances | Alcohol | Opioids | Cannabis | Stimulants | Alcohol | Opioids | Cannabis | Stimulants | |
| United States | 119 | 68 | 23 | 17 | 17 | —c | —c | —c | —c |
| Rhode Island | 165 | 98 | 35 | 22 | 18 | 80.0 | 40.0 | 40.0 | 20.0 |
| Massachusetts | 157 | 95 | 39 | 18 | 16 | 71.4 | 64.3 | 28.6 | 28.6 |
| California | 156 | 86 | 27 | 21 | 32 | 22.4 | 19.3 | 26.3 | 62.5 |
| Oregon | 155 | 84 | 37 | 21 | 26 | 33.3 | 18.5 | 35.7 | 44.4 |
| Washington | 150 | 73 | 44 | 22 | 24 | 8.6 | 42.9 | 37.1 | 42.9 |
| Minnesota | 143 | 89 | 26 | 23 | 16 | 27.1 | 11.7 | 21.3 | 17.8 |
| Maryland | 143 | 78 | 41 | 24 | 20 | 35.0 | 50.0 | 40.0 | 25.0 |
| Hawaii | 136 | 66 | 23 | 26 | 36 | 0.0 | 0.0 | 25.0 | 50.0 |
| Arizona | 135 | 73 | 26 | 17 | 20 | 38.5 | 15.4 | 7.7 | 46.2 |
| West Virginia | 130 | 70 | 33 | 14 | 6 | 25.5 | 65.5 | 20.0 | 2.2 |
| New Mexico | 129 | 79 | 26 | 17 | 16 | 41.9 | 10.3 | 27.6 | 44.8 |
| Michigan | 127 | 74 | 23 | 26 | 13 | 28.9 | 11.0 | 25.3 | 2.8 |
| New Jersey | 125 | 71 | 31 | 16 | 16 | 42.1 | 63.2 | 31.6 | 31.6 |
| Wisconsin | 123 | 82 | 19 | 13 | 10 | 34.7 | 9.7 | 14.1 | 6.0 |
| Florida | 123 | 71 | 21 | 17 | 16 | 59.0 | 27.9 | 37.7 | 27.9 |
| Kentucky | 117 | 61 | 27 | 14 | 9 | 17.5 | 51.8 | 24.8 | 5.7 |
| Wyoming | 114 | 79 | 14 | 13 | 10 | 10.0 | 0.0 | 11.1 | 0.0 |
| Nevada | 113 | 63 | 21 | 13 | 16 | 50.0 | 0.0 | 0.0 | 33.3 |
| Illinois | 111 | 67 | 20 | 17 | 14 | 12.7 | 4.1 | 24.8 | 12.0 |
| Pennsylvania | 107 | 61 | 24 | 11 | 12 | 22.7 | 31.8 | 13.6 | 3.3 |
| North Carolina | 103 | 57 | 17 | 16 | 15 | 29.6 | 35.1 | 44.9 | 56.1 |
| Indiana | 102 | 60 | 20 | 14 | 9 | 10.7 | 9.5 | 10.8 | 3.8 |
| Indiana | 102 | 60 | 20 | 14 | 9 | 10.7 | 9.5 | 10.8 | 3.8 |
| South Carolina | 101 | 63 | 13 | 14 | 13 | 27.9 | 4.7 | 23.3 | 30.2 |
| North Dakota | 99 | 65 | 16 | 12 | 9 | 9.5 | 9.1 | 15.4 | 18.2 |
| Tennessee | 96 | 47 | 25 | 12 | 9 | 25.8 | 61.3 | 12.9 | 3.6 |
| Oklahoma | 86 | 46 | 12 | 11 | 11 | 2.7 | 3.0 | 2.9 | 21.1 |
| Texas | 81 | 47 | 10 | 10 | 12 | 2.7 | 0.0 | 4.7 | 16.3 |
| Arkansas | 73 | 37 | 11 | 9 | 9 | 0.0 | 0.0 | 18.8 | 22.2 |
| Iowa | 68 | 45 | 7 | 6 | 6 | 0.0 | 0.0 | 0.0 | 1.4 |
| Louisiana | 65 | 34 | 10 | 10 | 9 | 0.0 | 5.6 | 0.0 | 22.2 |
| Utah | 55 | 25 | 16 | 7 | 9 | 0.0 | 4.5 | 0.0 | 5.3 |
| a The cost per capita (cost per 1 individual in the population) was calculated annually for each State and then averaged across the 3 years, weighted by the population total. b Hot spots were defined as counties with a substance-related inpatient stay rate in the highest quintile (top 20 percent). cNot calculated because not all States provide county-level data for Community-Level Statistics Note: Inpatient stays may involve more than one type of substance. Thus, substance-specific costs may sum to more than the cost for all substances combined. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), 2013--2015 National Inpatient Sample (NIS) and 2013-2015 State Inpatient Databases (SID) for 31 States, which, at the time this Statistical Brief was written, released data through the Community-Level Statistics pathway on HCUPnet, an online query tool. | |||||||||
| Table 3. Definition of substance use | ||
| ICD-9-CM description | ICD-9-CM code | Type of substance or substance-related condition |
|---|---|---|
| Chapter 5: Mental disorders (290-319) | ||
| Alcohol-induced mental disorders (291) | ||
| Alcohol withdrawal delirium | 291.0 | Alcohol |
| Alcohol-induced persisting amnestic disorder | 291.1 | Alcohol |
| Alcohol-induced persisting dementia | 291.2 | Alcohol |
| Alcohol-induced psychotic disorder with hallucinations | 291.3 | Alcohol |
| Idiosyncratic alcohol intoxication | 291.4 | Alcohol |
| Alcohol-induced psychotic disorder with delusions | 291.5 | Alcohol |
| Other specified alcohol-induced mental disorders | ||
| Alcohol withdrawal | 291.81 | Alcohol |
| Alcohol-induced sleep disorders | 291.82 | Alcohol |
| Other alcohol-induced mental disorders | 291.89 | Alcohol |
| Unspecified alcohol-induced mental disorder | 291.9 | Alcohol |
| Drug-induced mental disorders (292) | ||
| Drug withdrawal | 292.0 | Drug-induced mental disorders |
| Drug-induced psychotic disorders with delusions | 292.11 | Drug-induced mental disorders |
| Drug-induced psychotic disorders with hallucinations | 292.12 | Drug-induced mental disorders |
| Pathological drug intoxication | 292.2 | Drug-induced mental disorders |
| Drug-induced delirium | 292.81 | Drug-induced mental disorders |
| Drug-induced persisting dementia | 292.82 | Drug-induced mental disorders |
| Drug-induced amnestic disorder | 292.83 | Drug-induced mental disorders |
| Drug-induced mood disorder | 292.84 | Drug-induced mental disorders |
| Drug-induced sleep disorders | 292.85 | Drug-induced mental disorders |
| Other specified drug-induced mental disorders | 292.89 | Drug-induced mental disorders |
| Unspecified drug-induced mental disorder | 292.9 | Drug-induced mental disorders |
| Alcohol and drug dependence (303, 304) | ||
| Acute alcohol intoxication | 303.0x | Alcohol |
| Other and unspecified alcohol dependence | 303.9x | Alcohol |
| Opioid type dependence | 304.0x | Opioids |
| Sedative, hypnotic or anxiolytic dependence | 304.1x | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Cocaine dependence | 304.2x | Stimulants |
| Cannabis dependence | 304.3x | Cannabis |
| Amphetamine and other psychostimulant dependence | 304.4x | Stimulants |
| Hallucinogen dependence | 304.5x | Hallucinogens |
| Other specified drug dependence (absinthe, glue, inhalant, phencyclidine) | 304.6x | Other |
| Combinations of opioid type drug with any other drug dependence | 304.7x | Opioids |
| Combinations of drug dependence excluding opioid type drug | 304.8x | Other |
| Unspecified drug dependence | 304.9x | Other |
| Nondependent abuse of drugs (305) | ||
| Nondependent alcohol abuse | 305.0x | Alcohol |
| Nondependent cannabis abuse | 305.2x | Cannabis |
| Nondependent hallucinogen abuse | 305.3x | Hallucinogens |
| Nondependent sedative, hypnotic or anxiolytic abuse | 305.4x | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Nondependent opioid abuse | 305.5x | Opioids |
| Nondependent cocaine abuse | 305.6x | Stimulants |
| Nondependent amphetamine or related acting sympathomimetic abuse | 305.7x | Stimulants |
| Nondependent anti-depressant abuse | 305.8x | Other |
| Nondependent other mixed or unspecified drug abuse | 305.9x | Other |
| Chapters 6, 7, and 9: Diseases of the nervous system and sense organs (320-389), Diseases of the circulatory system (390-459), and Diseases of the digestive system (520-579) | ||
| Alcoholic polyneuropathy | 357.5 | Alcohol |
| Alcoholic cardiomyopathy | 425.5 | Alcohol |
| Alcoholic gastritis, without mention of hemorrhage | 535.30 | Alcohol |
| Alcoholic gastritis, with hemorrhage | 535.31 | Alcohol |
| Fatty liver | 571.0 | Alcohol |
| Acute alcoholic hepatitis | 571.1 | Alcohol |
| Alcoholic cirrhosis of liver | 571.2 | Alcohol |
| Alcoholic liver damage unspecified | 571.3 | Alcohol |
| Chapter 11: Complications of pregnancy, childbirth and the puerperium (630-679) | ||
| Drug dependence complicating pregnancy | 648.3x | Other |
| Chapter 15: Newborn (perinatal) (760-779) | ||
| Noxious influences affecting fetus or newborn via placenta or breastmilk (760) | ||
| Fetal alcohol syndrome | 760.71 | Alcohol |
| Narcotics affecting newborn | 760.72 | Opioids |
| Hallucinogens affecting newborn | 760.73 | Hallucinogens |
| Cocaine affecting newborn | 760.75 | Stimulants |
| Other and ill-defined conditions originating in the perinatal period (779) | ||
| Drug withdrawal syndrome in newborn | 779.5 | Opioids |
| Chapter 17: Injury and poisoning (800-999) | ||
| Poisoning by drugs, medicinal substances, and biologicals (960-979) | ||
| Opium (alkaloids) | 965.00 | Opioids |
| Heroin | 965.01 | Opioids |
| Methadone | 965.02 | Opioids |
| Other opiates and related narcotics | 965.09 | Opioids |
| Barbiturates | 967.0 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Chloral hydrate group | 967.1 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Paraldehyde | 967.2 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Bromine compounds | 967.3 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Methaqualone compounds | 967.4 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Glutethimide group | 967.5 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Mixed sedatives, not elsewhere classified | 967.6 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Other sedatives and hypnotics | 967.8 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Unspecified sedative or hypnotic (sleeping pills) | 967.9 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Surface [topical] and infiltration anesthetics | 968.59 | Stimulants |
| Benzodiazepine-based tranquilizers | 969.4 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Other tranquilizer | 969.5 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Hallucinogens | 969.6 | Hallucinogens |
| Psychostimulant NOS (Begin 2009) | 969.70 | Stimulants |
| Amphetamine (Begin 2009) | 969.72 | Stimulants |
| Methylphendate (Begin 2009) | 969.73 | Stimulants |
| Psychostimulant NEC (Begin 2009) | 969.79 | Stimulants |
| Opiate antagonist | 970.1 | Opioids |
| CNS stimulant NEC (only 2006-2010) | 970.8 | Stimulants |
| Cocaine (Begin 2010) | 970.81 | Stimulants |
| CNS stimulant NEC (Begin 2010) | 970.89 | Stimulants |
| CNS stimulant NOS | 970.9 | Stimulants |
| Antitussives | 975.4 | Other |
| Anti-common cold drugs | 975.6 | Other |
| Ethyl alcohol | 980.0 | Alcohol |
| Other specified alcohols | 980.8 | Alcohol |
| Unspecified alcohol | 980.9 | Alcohol |
| Supplemental classification of external causes of injury and poisoning (E-Codes) | ||
| Accidental poisoning by drugs, medicinal substances, and biologicals (E850-E858) | ||
| Accidental poisoning by heroin | E850.0 | Opioids |
| Accidental poisoning by methadone | E850.1 | Opioids |
| Accidental poisoning by other opiates and related narcotics | E850.2 | Opioids |
| Accidental poisoning by barbiturates | E851 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Chlorl hydrate | E852.0 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Paraldehyde | E852.1 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Bromine compound | E852.2 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Methaqualone compounds | E852.3 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Glutethimide group | E852.4 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Mixed sedatives NEC | E852.5 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Other specified sedatives and hypnotics | E852.8 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Unspecified sedative or hypnotic | E852.9 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Benzodiazepine-based tranquilizers | E853.2 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Tranquilizer NEC | E853.8 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Tranquilizer NOS | E853.9 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Accidental poisoning by hallucinogens | E854.1 | Hallucinogens |
| Accidental poisoning by psychostimulants | E854.2 | Stimulants |
| Accidental poisoning by central nervous system stimulants (analeptics, opiate antagonists) | E854.3 | Stimulants |
| Accidental poisoning by other solid and liquid substances, gases, and vapors (E860-E869) | ||
| Alcohol beverage | E860.0 | Alcohol |
| Ethyl alcohol | E860.1 | Alcohol |
| Alcohol NEC | E860.8 | Alcohol |
| Alcohol NOS | E860.9 | Alcohol |
| Drugs, medicinal substances, and biologicals causing adverse effects in therapeutic use (E930-E949) | ||
| Heroin causing adverse effects in therapeutic use | E935.0 | Opioids |
| Suicide and self-inflicted poisoning by solid or liquid substances (E950) | ||
| Suicide and self-inflicted poisoning by barbiturates | E950.1 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Suicide and self-inflicted poisoning by other sedatives/hypnotics | E950.2 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Suicide and self-inflicted poisoning by tranquilizers and other psychotropic agents | E950.3 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Poisoning by solid or liquid substances, undetermined whether accidentally or purposely inflicted (E980-E989) | ||
| Undetermined poisoning by barbiturates | E980.1 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Undetermined poisoning by other sedatives and hypnotics | E980.2 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Undetermined poisoning by tranquilizers and other psychotropic agents | E980.3 | Sedatives, hypnotics, anxiolytics, tranquilizers, barbiturates |
| Classification of factors influencing health status and contact with health services (V-Codes) | ||
| Counseling, substance use | V65.42 | Other |
| Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; NEC, not elsewhere classifiable; NOS, not otherwise specified | ||
| Supplemental Table 1. County-level variation in rates of alcohol-related inpatient stays, by State, 2013-2015, for data presented in Figure 1 | |||||
| State (Number of Counties) | County With Minimum Rate | State Mean Rate | County With Maximum Rate | ||
|---|---|---|---|---|---|
| County | Rate | County | Rate | ||
| Massachusetts (N=14) | Nantucket | 635 | 897 | Berkshire | 1,087 |
| Rhode Island (N=5) | Bristol | 617 | 802 | Providence | 960 |
| Florida (N=61) | Lafayette | 258 | 711 | Monroe | 1,494 |
| Maryland (N=20) | Howard | 337 | 685 | Baltimore City | 1,955 |
| Arizona (N=13) | Santa Cruz | 286 | 665 | Graham | 1,132 |
| Wisconsin (N=72) | Grant | 247 | 660 | Menominee | 1,987 |
| New Mexico (N=31) | Los Alamos | 401 | 659 | Rio Arriba | 1,169 |
| Nevada (N=16) | Lincoln | 294 | 655 | Mineral | 1,369 |
| North Carolina (N=98) | Jones | 268 | 619 | Swain | 1,393 |
| New Jersey (N=19) | Bergen | 334 | 615 | Cape May | 876 |
| Michigan (N=83) | Ottowa | 282 | 604 | Keweenaw | 1,390 |
| West Virginia (N=55) | Gilmer | 278 | 598 | Mercer | 989 |
| Minnesota (N=85) | Red Lake | 249 | 592 | Cass | 1,275 |
| Oregon (N=30) | Hood River | 333 | 591 | Wheeler | 941 |
| South Carolina (N=43) | Pickens | 333 | 581 | Lee | 845 |
| Tennessee (N=31) | Williamson | 247 | 578 | Washington | 1,083 |
| North Dakota (N=21) | Oliver | 310 | 571 | Sioux | 2,725 |
| California (N=58) | Kings | 320 | 569 | Lake | 1,192 |
| Pennsylvania (N=66) | Clinton | 246 | 555 | Allegheny | 998 |
| Wyoming (N=10) | Uinta | 326 | 512 | Laramie | 827 |
| Washington (N=35) | Adams | 212 | 503 | Grays Harbor | 760 |
| Kentucky (N=114) | Allen | 233 | 501 | Perry | 1,523 |
| Illinois (N=102) | Edwards | 233 | 489 | Rock Island | 952 |
| Indiana (N=84) | La Grange | 208 | 456 | Vanderburgh | 815 |
| Hawaii (N=4) | Honolulu | 346 | 438 | Hawaii | 534 |
| Oklahoma (N=74) | Major | 173 | 429 | Kiowa | 744 |
| Arkansas (N=64) | Sevier | 197 | 414 | Garland | 646 |
| Texas (N=147) | Kendall | 139 | 402 | Potter | 1,104 |
| Louisiana (N=19) | St. James Parish | 234 | 351 | Cameron Parish | 570 |
| Iowa (N=90) | Davis | 141 | 350 | Scott | 656 |
| Utah (N=26) | Utah | 136 | 254 | Weber | 478 |
| Supplemental Table 2. County-level variation in rates of opioid-related inpatient stays, by State, 2013-2015, for data presented in Figure 2 | |||||
| State (Number of Counties) | County With Minimum Rate | State Mean Rate | County With Maximum Rate | ||
|---|---|---|---|---|---|
| County | Rate | County | Rate | ||
| Massachusetts (N=14) | Nantucket | 179 | 399 | Berkshire | 1,091 |
| West Virginia (N=55) | Calhoun | 94 | 353 | McDowell | 695 |
| Kentucky (N=112) | Trigg | 38 | 352 | Owsley | 1,220 |
| Tennessee (N=31) | Williamson | 80 | 349 | Carter | 759 |
| Maryland (N=20) | Prince George's | 95 | 348 | Baltimore City | 1,592 |
| New Jersey (N=19) | Bergen | 109 | 314 | Atlantic | 577 |
| Rhode Island (N=5) | Washington | 189 | 269 | Providence | 391 |
| Washington (N=35) | Adams | 54 | 259 | Grays Harbor | 543 |
| Pennsylvania (N=66) | Union | 90 | 245 | Armstrong | 503 |
| North Carolina (N=97) | Hertford | 53 | 238 | Swain | 745 |
| Florida (N=61) | Hardee | 53 | 216 | Bradford | 495 |
| Oregon (N=27) | Benton | 69 | 212 | Multnomah | 479 |
| California (N=57) | San Benito | 67 | 210 | Toulumne | 759 |
| New Mexico (N=29) | Hidalgo | 86 | 196 | Rio Arriba | 611 |
| Indiana (N=84) | La Grange | 27 | 188 | Jackson | 1,028 |
| Nevada (N=12) | Humboldt | 62 | 181 | Carson City | 274 |
| Michigan (N=82) | Ottowa | 58 | 181 | Wayne | 415 |
| Arizona (N=13) | Santa Cruz | 67 | 181 | Mohave | 330 |
| North Dakota (N=11) | Stutsman | 62 | 181 | Sioux | 751 |
| Wisconsin (N=72) | Grant | 40 | 160 | Ashland | 458 |
| Minnesota (N=77) | Yellow Medicine | 41 | 156 | Mahnomen | 985 |
| Utah (N=22) | Grand | 40 | 142 | Weber | 290 |
| Oklahoma (N=66) | Woodward | 38 | 142 | Adair | 434 |
| Louisiana (N=18) | St. James Parish | 34 | 141 | Livingston Parish | 328 |
| Hawaii (N=4) | Kauai | 87 | 141 | Maui | 193 |
| South Carolina (N=43) | Allendale | 40 | 130 | Georgetown | 361 |
| Illinois (N=97) | Jo Daviess | 43 | 127 | Cook | 426 |
| Arkansas (N=64) | Bradley | 48 | 122 | Crawford | 244 |
| Wyoming (N=9) | Goshen | 55 | 112 | Washakie | 166 |
| Texas (N=120) | Starr | 15 | 74 | Nueces | 227 |
| Iowa (N=67) | Buchanan | 18 | 55 | Marshall | 169 |
| Figure 3. County-level variation in rates of cannabis-related inpatient stays, by State, 2013-2015 | |||||
| State (Number of Counties) | County With Minimum Rate | State Mean Rate | County With Maximum Rate | ||
|---|---|---|---|---|---|
| County | Rate | County | Rate | ||
| Maryland (N=20) | Montgomery | 103 | 245 | Baltimore City | 843 |
| Massachusetts (N=14) | Norfolk | 98 | 230 | Berkshire | 736 |
| North Carolina (N=98) | Onslow | 63 | 222 | Robeson | 635 |
| Hawaii (N=4) | Kauai | 79 | 206 | Hawaii | 446 |
| Rhode Island (N=5) | Washington | 130 | 205 | Providence | 294 |
| Michigan (N=83) | Leelanau | 62 | 195 | Genesee | 647 |
| California (N=57) | Colusa | 64 | 191 | Trinity | 557 |
| Oregon (N=28) | Hood River | 77 | 190 | Multnomah | 291 |
| New Mexico (N=29) | Los Alamos | 98 | 189 | Quay | 276 |
| Florida (N=61) | Lafayette | 56 | 189 | Escambia | 420 |
| Washington (N=35) | Adams | 57 | 189 | Lewis | 355 |
| Illinois (N=101) | Jo Daviess | 31 | 185 | Marion | 498 |
| Minnesota (N=80) | Marshall | 52 | 181 | Mahnomen | 563 |
| South Carolina (N=43) | Oconee | 67 | 179 | Darlington | 308 |
| New Jersey (N=19) | Bergen | 66 | 178 | Camden | 326 |
| North Dakota (N=13) | Stutsman | 71 | 178 | Sioux | 697 |
| Kentucky (N=113) | Barren | 42 | 164 | Kenton | 481 |
| West Virginia (N=55) | Wirt | 80 | 162 | Ohio | 326 |
| Arkansas (N=64) | Sevier | 43 | 149 | Jefferson | 318 |
| Arizona (N=13) | Santa Cruz | 61 | 142 | Mohave | 229 |
| Tennessee (N=31) | Williamson | 40 | 140 | Washington | 378 |
| Pennsylvania (N=66) | Wyoming | 46 | 137 | Armstrong | 350 |
| Indiana (N=83) | Cass | 47 | 134 | Vanderburgh | 346 |
| Wisconsin (N=71) | Grant | 30 | 127 | Menominee | 403 |
| Oklahoma (N=70) | Major | 51 | 126 | Comanche | 230 |
| Nevada (N=13) | Lincoln | 77 | 126 | Churchill | 182 |
| Wyoming (N=9) | Big Horn | 46 | 122 | Laramie | 227 |
| Louisiana (N=18) | St. Tammany Parish | 61 | 121 | West Baton Rouge Parish | 179 |
| Texas (N=129) | Val Verde | 19 | 109 | Potter | 376 |
| Utah (N=19) | Carbon | 36 | 73 | Weber | 204 |
| Iowa (N=67) | Carroll | 22 | 64 | Pottawattamie | 207 |
| Figure 4. County-level variation in rates of stimulant-related inpatient stays, by State, 2013-2015 | |||||
| State (Number of Counties) | County With Minimum Rate | State Mean Rate | County With Maximum Rate | ||
|---|---|---|---|---|---|
| County | Rate | County | Rate | ||
| California (N=56) | Mono | 52 | 222 | Lake | 556 |
| Hawaii (N=4) | Maui | 137 | 213 | Honolulu | 309 |
| New Mexico (N=29) | Los Alamos | 48 | 182 | Chaves | 428 |
| North Carolina (N=98) | Onslow | 43 | 181 | Halifax | 481 |
| Oregon (N=27) | Hood River | 78 | 175 | Multnomah | 373 |
| Maryland (N=20) | Garrett | 41 | 174 | Baltimore City | 931 |
| Washington (N=35) | Adams | 59 | 169 | Grays Harbor | 391 |
| Massachusetts (N=14) | Dukes | 63 | 167 | Berkshire | 495 |
| Arizona (N=13) | Santa Cruz | 49 | 150 | Graham | 257 |
| Nevada (N=12) | Humboldt | 90 | 149 | Carson City | 218 |
| South Carolina (N=43) | Oconee | 63 | 148 | Orangeburg | 262 |
| New Jersey (N=19) | Sussex | 55 | 148 | Camden | 328 |
| Florida (N=61) | Sumter | 53 | 146 | Escambia | 403 |
| Arkansas (N=63) | Benton | 59 | 138 | Woodruff | 332 |
| Rhode Island (N=5) | Washington | 66 | 133 | Providence | 237 |
| Oklahoma (N=71) | Kingfisher | 46 | 129 | Kiowa | 262 |
| North Dakota (N=11) | Richland | 48 | 120 | Sioux | 449 |
| Minnesota (N=73) | Roseau | 39 | 119 | Mahnomen | 429 |
| Louisiana (N=18) | Plaquemines Parish | 32 | 111 | Terrebonne Parish | 234 |
| Texas (N=129) | Val Verde | 23 | 110 | Potter | 488 |
| Illinois (N=92) | Warren | 29 | 93 | Marion | 291 |
| Utah (N=19) | Wasatch | 35 | 84 | Weber | 271 |
| Kentucky (N=105) | Calloway | 29 | 82 | Fayette | 191 |
| Tennessee (N=28) | Williamson | 26 | 82 | Davidson | 206 |
| Wyoming (N=9) | Big Horn | 37 | 79 | Laramie | 161 |
| Pennsylvania (N=61) | Wayne | 18 | 77 | Philadelphia | 469 |
| West Virginia (N=45) | Jackson | 29 | 70 | Ohio | 195 |
| Wisconsin (N=67) | Oconto | 12 | 68 | Milwaukee | 294 |
| Indiana (N=80) | Franklin | 24 | 66 | Marion | 186 |
| Michigan (N=71) | Charlevoix | 16 | 66 | Wayne | 315 |
| Iowa (N=69) | Winneshiek | 21 | 55 | Pottawattamie | 196 |
| Supplemental Table 5. Average cost per type of substance-related inpatient stay, by State, 2013-2015, for data presented in Figure 7 | |||||
| State | All Stays | Cannabis | Stimulants | Alcohol | Opioids |
|---|---|---|---|---|---|
| California | 14.9 | 12.4 | 14.3 | 17.2 | 17.2 |
| Hawaii | 13.9 | 13.0 | 12.9 | 16.5 | 17.5 |
| Washington | 13.4 | 12.0 | 13.4 | 14.8 | 14.7 |
| Oregon | 12.8 | 10.8 | 12.8 | 14.7 | 13.6 |
| Arizona | 10.6 | 10.4 | 11.0 | 12.9 | 11.8 |
| Nevada | 10.7 | 10.1 | 10.7 | 12.7 | 12.7 |
| Wyoming | 12.5 | 10.0 | 10.8 | 12.5 | 13.5 |
| Wisconsin | 11.6 | 8.8 | 9.9 | 12.4 | 10.9 |
| New Jersey | 11.5 | 9.3 | 10.5 | 12.1 | 10.6 |
| Minnesota | 11.7 | 9.9 | 10.3 | 12.1 | 12.2 |
| Texas | 10.3 | 8.7 | 9.6 | 12.0 | 12.1 |
| New Mexico | 10.2 | 9.2 | 9.3 | 11.7 | 11.4 |
| United States | 11.0 | 8.9 | 10.0 | 11.6 | 10.5 |
| Massachusetts | 11.9 | 9.2 | 9.9 | 11.4 | 10.4 |
| South Carolina | 10.5 | 8.3 | 9.0 | 11.4 | 9.7 |
| Indiana | 10.6 | 7.8 | 9.4 | 11.2 | 10.2 |
| Michigan | 10.2 | 8.8 | 9.3 | 11.0 | 9.16 |
| Rhode Island | 11.5 | 8.9 | 9.5 | 11.0 | 10.5 |
| Kentucky | 10.3 | 7.7 | 8.8 | 10.8 | 8.7 |
| Maryland | 11.1 | 8.8 | 9.4 | 10.8 | 9.9 |
| Iowa | 10.4 | 8.4 | 9.8 | 10.8 | 11.9 |
| Illinois | 10.6 | 7.3 | 7.9 | 10.5 | 7.5 |
| North Dakota | 10.4 | 7.4 | 8.0 | 10.3 | 10.8 |
| West Virginia | 10.6 | 7.2 | 7.6 | 10.3 | 8.3 |
| Pennsylvania | 10.2 | 7.0 | 8.3 | 10.0 | 8.6 |
| Florida | 9.5 | 7.7 | 8.1 | 10.0 | 9.8 |
| North Carolina | 9.9 | 7.3 | 7.9 | 9.9 | 8.3 |
| Oklahoma | 9.3 | 7.0 | 7.6 | 9.4 | 8.3 |
| Utah | 9.3 | 7.2 | 7.2 | 8.7 | 8.4 |
| Arkansas | 8.4 | 5.9 | 6.3 | 8.5 | 9.2 |
| Tennessee | 8.6 | 6.4 | 7.4 | 8.3 | 7.4 |
| Louisiana | 9.3 | 5.9 | 6.0 | 8.1 | 6.6 |