|
STATISTICAL BRIEF #298
October 2022
Marguerite L. Barrett, M.S., Pamela L. Owens, Ph.D., and Marc Roemer, M.S. Introduction In the United States in 2019, there were approximately 143 million emergency department (ED) visits, and about 14 percent of these ED visits resulted in hospitalization.1 At the start of the COVID-19 pandemic, ED utilization overall declined substantially, with a 42 percent decrease in ED visits in April 2020 compared with April 2019.2 Studies suggest patients may be avoiding care in the ED,3,4 including patients with serious conditions,5,6 or seeking other types of urgent care (e.g., telehealth).7 Although studies have examined the change in the volume of ED visits before versus during the COVID-19 pandemic for certain patient demographic groups and conditions,8-10 little is known about the variation in the type of conditions treated in the ED and change in the percentage of ED visits that result in hospitalization. This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents data on ED visits from 29 States based on the 2019 and 2020 State Emergency Department Databases (SEDD) and a subset of the State Inpatient Databases (SID) that includes information on ED visits that result in an admission to the same hospital. The initial period of the COVID-19 pandemic (April–December 2020) is compared with the same months of the prior year. ED visit volume and ED admission rate (defined as the percentage of ED visits that result in hospitalization) are presented for both time periods across all conditions and for COVID-19-related visits specifically. In addition, the variation in the ED admission rate across the 29 States is provided. Information on changes in ED visit volume and ED admission rate is presented by patient characteristics and for the conditions with the largest percentage increase and decrease between April–December 2019 and April–December 2020. Because the HCUP SID and SEDD cover nearly the entire universe of hospital encounters in a State, small differences can be evident but not meaningful. Thus, only differences greater than or equal to 10 percent are discussed in the text. This analysis is limited to ED visits in 29 States (Alaska, Arizona, California, Connecticut, Georgia, Hawaii, Illinois, Indiana, Iowa, Kansas, Kentucky, Maine, Maryland, Michigan, Minnesota, Mississippi, Montana, Nevada, North Carolina, North Dakota, Ohio, Oregon, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, and Wisconsin) for which HCUP SID and SEDD were available for April–December 2019 and April–December 2020. These States accounted for 61.5 percent of the resident U.S. population in 2020.11 Information contained in this Statistical Brief was primarily obtained from the HCUP Summary Trend Tables.12 The HCUP Summary Trend Tables, accessed as downloadable tables, provide State-specific monthly trends in hospital utilization for the most recent HCUP data available. These tables were also used to create the HCUP Visualization of Inpatient Trends in COVID-19 and Other Conditions13 and will be updated periodically as more data become available. |
|
Findings
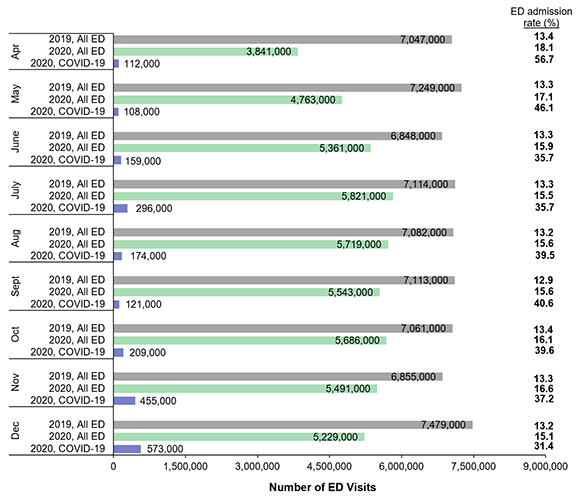
ED visit volume and ED admission rate in April–December 2019 and 2020 Figure 1 presents monthly information on ED visit volume and ED admission rate (percentage of ED visits that result in admission) overall in 2019 and 2020 and for ED visits related to COVID-19 in 2020. In total, there were 63,848,000 ED visits in April–December 2019 and 47,455,000 ED visits in April–December 2020. There were 2,208,000 COVID-19-related ED visits in April–December 2020, 37.4 percent of which resulted in admission. Figure 1. Number of ED visits and ED admission rate, by month and type of visit, 29 States, April–December 2019 and 2020
Bar chart that presents monthly information on emergency department (ED) visit volume and ED admission rate (percentage of ED visits that result in admission) overall in 2019 and 2020 and for ED visits related to COVID-19 in 2020. Data are provided in Supplemental Table 1.
|
|
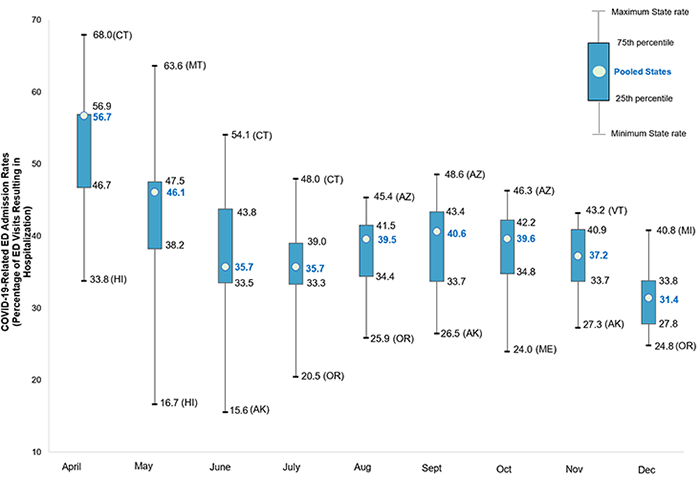
Figure 2 displays the monthly distribution of the State-specific COVID-19 ED admission rates (i.e., percentage of COVID-19-related ED visits that resulted in hospitalization). The figure shows the lowest State-specific ED admission rate (minimum) and the highest State-specific ED admission rate (maximum), as well as the interquartile range of the State-specific ED admission rates (blue box). The monthly ED admission rate using the aggregated data from the 29 States (pooled rate) is presented in blue text.
Figure 2. Variation in the State-specific rates of COVID-19-related ED visits resulting in hospitalization, by month, April–December 2020
Box plot that shows the monthly distribution of the State-specific COVID-19 emergency department (ED) admission rates (i.e., percentage of COVID-19-related ED visits that resulted in hospitalization), including the lowest State-specific ED admission rate (minimum), the highest State-specific ED admission rate (maximum), the interquartile range of the State-specific ED admission rates, and the monthly ED admission rate using the aggregated data from the 29 States (pooled rate). Data are provided in Supplemental Table 2.
|
|
Table 1 presents information on total ED visit volume and number of ED visits resulting in hospitalization by patient characteristic in April through December 2019 and 2020 across the 29 States.
Table 1. Number of ED visits, number of ED visits resulting in hospitalization, and percentage change, by patient characteristic, 29 States, April–December 2019 and 2020 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
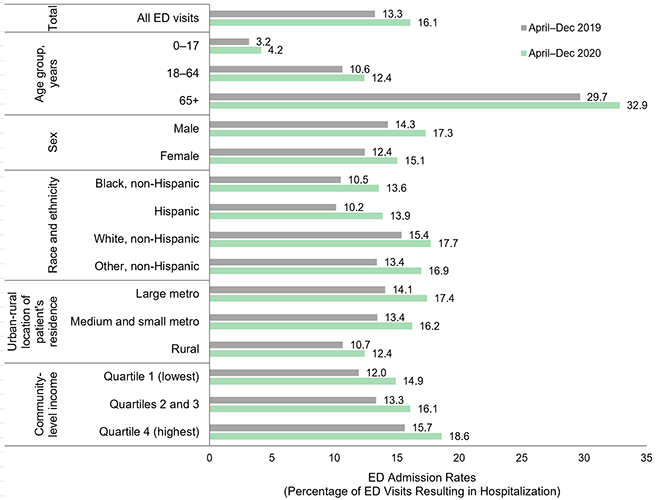
Figure 3 presents information on ED admission rates by patient characteristic in April through December 2019 and 2020 across the 29 States. The ED admission rate is defined as the percentage of ED visits that result in hospitalization.
Figure 3. ED admission rates, by patient characteristic, 29 States, April–December 2019 and 2020
Bar chart presenting emergency department (ED) admission rates by patient characteristic in April through December 2019 and 2020 across 29 States. Data are provided in Supplemental Table 3.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Changes in ED visit volume by condition in April–December 2019 and 2020
Tables 2 and 3 present information on ED visit volume in April–December 2019 and 2020 by select conditions. The ED visit volume for the five conditions with the greatest percentage change during this period is presented for treat-and-release ED visits (Table 2) and ED visits resulting in hospitalization (Table 3). Selection of conditions was made separately for first-listed/principal and all-listed diagnoses. Conditions listed have at least 10,000 ED visits in 2019 and at least a 10 percent change between 2019 and 2020. Each table displays the condition chiefly responsible for the ED service or hospitalization (first-listed or principal, respectively) and all-listed conditions that coexisted at the time of the ED visit or hospitalization. Hyphens indicate that a condition was not in the top five for the respective selection criteria (first-listed/principal and all-listed diagnoses). Table 2. Top five conditions with the greatest percentage change (more than 10 percent) in the number of treat-and-release ED visits, 29 States, April–December 2019 and 2020 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 3. Top five conditions with the greatest percentage change (more than 10 percent) in the number of ED visits resulting in hospitalization, 29 States, April–December 2019 and 2020
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
About Statistical Briefs
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Data Source
The estimates in this Statistical Brief are based upon data from the HCUP 2019–2020 State Emergency Department Databases (SEDD) and State Inpatient Databases (SID) for 29 States for which there were monthly data available through December 2020 in the HCUP Summary Trend Tables. The States included in this Statistical Brief were Alaska, Arizona, California, Connecticut, Georgia, Hawaii, Illinois, Indiana, Iowa, Kansas, Kentucky, Maine, Maryland, Michigan, Minnesota, Mississippi, Montana, Nevada, North Carolina, North Dakota, Ohio, Oregon, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, and Wisconsin. The SEDD include ED visits that do not result in admission to the same hospital, such as treat-and-release ED visits, transfers to other hospitals or health facilities, encounters during which the patient left against medical advice, and cases in which the patient died while receiving ED care. The SID capture inpatient stays, including those that originate in the ED and result in an admission to the same hospital. This Statistical Brief uses all records from the SEDD and the subset of SID records specific to ED admissions. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Definitions
Diagnoses, ICD-10-CM, and Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses
ICD-10-CM is the International Classification of Diseases, Tenth Revision, Clinical Modification. There are over 70,000 ICD-10-CM diagnosis codes. The CCSR aggregates ICD-10-CM diagnosis codes into a manageable number of clinically meaningful categories.d The CCSR is intended to be used analytically to examine patterns of healthcare in terms of cost, utilization, and outcomes; rank utilization by diagnoses; and risk-adjust by clinical condition. The CCSR capitalizes on the specificity of the ICD-10-CM coding scheme and allows ICD-10-CM codes to be classified in more than one category. Approximately 10 percent of diagnosis codes are associated with more than one CCSR category because the diagnosis code documents either multiple conditions or a condition along with a common symptom or manifestation. For this Statistical Brief, the principal/first-listed diagnosis code is assigned to a single default CCSR based on clinical coding guidelines, etiology and pathology of diseases, and standards set by other Federal agencies. The assignment of the default CCSR for the principal diagnosis is available starting with version v2020.2 of the software tool. The assignment of the default CCSR for the first-listed diagnosis for outpatient data is available starting with version v2021.1 of the software tool. ICD-10-CM coding definitions for each CCSR category presented in this Statistical Brief can be found in the CCSR reference file, available at www.hcup-us.ahrq.gov/toolssoftware/ccsr/ccs_refined.jsp#download. For this Statistical Brief, v2021.2 of the CCSR was used.
Case definition
Types of hospitals included in HCUP State Emergency Department Databases
Types of hospitals included in HCUP State Inpatient Databases
Unit of analysis
Percentage change
Percentage change between groups equals the 2020 value minus the 2019 value divided by the 2019 value and multiplied by 100.
Reporting of race and ethnicity
Location of patients’ residence
Community-level income
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels.
HCUP would not be possible without the contributions of the following data collection Partners from across the United States:
|
Alaska Department of Health Alaska Hospital and Healthcare Association Arizona Department of Health Services Arkansas Department of Health California Department of Health Care Access and Information Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Laulima Data Alliance Hawaii University of Hawai'i at Hilo Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services |
New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association |
The HCUP State Emergency Department Databases (SEDD) include information from hospital-owned emergency departments (EDs) from data organizations participating in HCUP, translated into a uniform format to facilitate multistate comparisons and analyses. The SEDD capture the universe of records on ED visits in participating HCUP States that do not result in an admission to the same hospital (i.e., encounters for patients who are treated in the ED and then released in the ED, transferred to another hospital or health facility, left against medical advice, or died while receiving ED care). The SEDD contain a core set of clinical and nonclinical information on all patients, including individuals covered by Medicare, Medicaid, or private insurance, as well as those whose stays were not expected to be covered by insurance. The SEDD can be used to investigate questions unique to one State, to compare data from two or more States, to conduct market-area variation analyses, and to identify State-specific trends in injury surveillance, emerging infections, and other conditions treated in the ED.
The HCUP State Inpatient Databases (SID) are hospital inpatient databases from data organizations participating in HCUP. The SID contain the universe of the inpatient discharge abstracts in the participating HCUP States, translated into a uniform format to facilitate multistate comparisons and analyses. Together, the SID encompass more than 95 percent of all U.S. community hospital discharges. The SID capture information on all types of inpatient discharges, including those admitted through the emergency department of the hospital, direct admissions, and transfers from acute care hospitals and other types of health facilities. The SID can be used to investigate questions unique to one State, to compare data from two or more States, to conduct market-area variation analyses, and to identify State-specific trends in inpatient care utilization, access, charges, and outcomes.
For other information on COVID-19, refer to the COVID-19 HCUP Statistical Briefs topic area located at www.hcup-us.ahrq.gov/reports/statbriefs/sbtopic.jsp.
For additional HCUP statistics, visit:
For more information about HCUP, visit www.hcupnet.ahrq.gov/.
For a detailed description of HCUP and more information on the design of the State Emergency Department Databases (SEDD) and State Inpatient Databases (SID), please refer to the following database documentation:
Agency for Healthcare Research and Quality. Overview of the State Emergency Department Databases (SEDD). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated September 2021. www.hcup-us.ahrq.gov/seddoverview.jsp. Accessed March 9, 2022.
Agency for Healthcare Research and Quality. Overview of the State Inpatient Databases (SID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated September 2021. www.hcup-us.ahrq.gov/sidoverview.jsp. Accessed March 9, 2022.
Barrett ML (M.L. Barrett, Inc.), Owens PL (AHRQ), Roemer, M (AHRQ). Changes in Emergency Department Visits in the Initial Period of the COVID-19 Pandemic (April–December 2020), 29 States. HCUP Statistical Brief #298. October 2022. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb298-COVID-19-ED-visits.pdf.
The authors would like to acknowledge the contributions of Molly Hensche, Brendan Leonard, Minya Sheng, and Jennifer Welch of IBM.
***
AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please email us at hcup@ahrq.gov. or send a letter to the address below:
Joel W. Cohen, Ph.D., Director
Center for Financing, Access and Cost Trends
Agency for Healthcare Research and Quality
5600 Fishers Lane
Rockville, MD 20857
This Statistical Brief was posted online on October 18, 2022.
a Centers for Medicare & Medicaid Services. ICD-10-CM Official Guidelines for Coding and Reporting FY 2022, Section IV-G. Updated April 1, 2022. www.cms.gov/files/document/fy-2022-icd-10-cm-coding-guidelines.pdf. Accessed September 2, 2022.
b Centers for Medicare & Medicaid Services. ICD-10-CM Official Guidelines for Coding and Reporting FY 2022, Section II. Updated April 1, 2022. www.cms.gov/files/document/fy-2022-icd-10-cm-coding-guidelines.pdf. Accessed September 2, 2022.
c Centers for Medicare & Medicaid Services. ICD-10-CM Official Guidelines for Coding and Reporting FY 2022, Section III. Updated April 1, 2022. www.cms.gov/files/document/fy-2022-icd-10-cm-coding-guidelines.pdf. Accessed September 2, 2022.
d Agency for Healthcare Research and Quality. Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses. Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality. Updated February 2022. www.hcup-us.ahrq.gov/toolssoftware/ccsr/dxccsr.jsp. Accessed September 2, 2022.
e Centers for Disease Control and Prevention, National Center for Health Statistics. ICD-10-CM Official Guidelines for Coding and Reporting FY 2021 (October 1, 2020 – September 30, 2021). www.cdc.gov/nchs/data/icd/10cmguidelines-FY2021.pdf. Accessed September 2, 2022.
f Claritas. Claritas Demographic Profile by ZIP Code. https://claritas360.claritas.com/mybestsegments/. Accessed September 2, 2022.
| Supplemental Table 1. Number of ED visits and ED admission rate, by month and type of visit, 29 States, April–December 2019 and 2020, for data presented in Figure 1 | |||
| Month | Visit type | All ED visits | % ED admission |
|---|---|---|---|
| April | 2019, All ED | 7,047,000 | 13.4 |
| 2020, All ED | 3,841,000 | 18.1 | |
| 2020, COVID-19 | 112,000 | 56.7 | |
| May | 2019, All ED | 7,249,000 | 13.3 |
| 2020, All ED | 4,763,000 | 17.1 | |
| 2020, COVID-19 | 108,000 | 46.1 | |
| June | 2019, All ED | 6,848,000 | 13.3 |
| 2020, All ED | 5,361,000 | 15.9 | |
| 2020, COVID-19 | 159,000 | 35.7 | |
| July | 2019, All ED | 7,114,000 | 13.3 |
| 2020, All ED | 5,821,000 | 15.5 | |
| 2020, COVID-19 | 296,000 | 35.7 | |
| August | 2019, All ED | 7,082,000 | 13.2 |
| 2020, All ED | 5,719,000 | 15.6 | |
| 2020, COVID-19 | 174,000 | 39.5 | |
| September | 2019, All ED | 7,113,000 | 12.9 |
| 2020, All ED | 5,543,000 | 15.6 | |
| 2020, COVID-19 | 121,000 | 40.6 | |
| October | 2019, All ED | 7,061,000 | 13.4 |
| 2020, All ED | 5,686,000 | 16.1 | |
| 2020, COVID-19 | 209,000 | 39.6 | |
| November | 2019, All ED | 6,855,000 | 13.3 |
| 2020, All ED | 5,491,000 | 16.6 | |
| 2020, COVID-19 | 455,000 | 37.2 | |
| December | 2019, All ED | 7,479,000 | 13.2 |
| 2020, All ED | 5,229,000 | 15.1 | |
| 2020, COVID-19 | 573,000 | 31.4 | |
| Supplemental Table 2. Variation in the State-specific rates of COVID-19-related ED visits resulting in hospitalization, by month, April–December 2020, for data presented in Figure 2 | |||||
| Month | Pooled States | 25th percentile | 75th percentile | Low | High |
|---|---|---|---|---|---|
| April | 56.7 | 46.7 | 56.9 | 33.8 (HI) | 68.0 (CT) |
| May | 46.1 | 38.2 | 47.5 | 16.7 (HI) | 63.6 (MT) |
| June | 35.7 | 33.5 | 43.8 | 15.6 (AK) | 54.1 (CT) |
| July | 35.7 | 33.3 | 39.0 | 20.5 (OR) | 48.0 (CT) |
| August | 39.5 | 34.4 | 41.5 | 25.9 (OR) | 45.4 (AZ) |
| September | 40.6 | 33.7 | 43.4 | 26.5 (AK) | 48.6 (AZ) |
| October | 39.6 | 34.8 | 42.2 | 24.0 (ME) | 46.3 (AZ) |
| November | 37.2 | 33.7 | 40.9 | 27.3 (AK) | 43.2 (VT) |
| December | 31.4 | 27.8 | 33.8 | 24.8 (OR) | 40.8 (MI) |
| Supplemental Table 3. ED admission rates, by patient characteristic, 29 States, April–December 2019 and 2020, for data presented in Figure 3 | ||
| Characteristic | April–Dec 2019 | April–Dec 2020 |
|---|---|---|
| Total: All ED visits | 13.3 | 16.1 |
| Age group, years | ||
| 0–17 | 3.2 | 4.2 |
| 18–64 | 10.6 | 12.4 |
| 65+ | 29.7 | 32.9 |
| Sex | ||
| Male | 14.3 | 17.3 |
| Female | 12.4 | 15.1 |
| Race and ethnicity | ||
| Black, non-Hispanic | 10.5 | 13.6 |
| Hispanic | 10.2 | 13.9 |
| White, non-Hispanic | 15.4 | 17.7 |
| Other, non-Hispanic | 13.4 | 16.9 |
| Urban-rural location of patient's residence | ||
| Large metro | 14.1 | 17.4 |
| Medium and small metro | 13.4 | 16.2 |
| Rural | 10.7 | 12.4 |
| Community-level income | ||
| Quartile 1 (lowest) | 12.0 | 14.9 |
| Quartiles 2 and 3 | 13.3 | 16.1 |
| Quartile 4 (highest) | 15.7 | 18.6 |