|
STATISTICAL BRIEF #304
September 2023
H. Joanna Jiang, Ph.D., and Molly Hensche, M.S. Introduction Hospital readmissions are one of the key measures used for evaluating the quality of inpatient care and post-discharge outpatient care. Although in most cases readmissions are necessary, a significant portion may be preventable. Strategies have been implemented at both the national and State levels to reduce preventable readmissions, particularly through improved discharge planning and care coordination. Hospitals and health systems are incentivized to implement these strategies by linking payment with certain key readmission measures. When the COVID-19 pandemic began in early 2020, hospital utilization decreased while the number of all-cause in-hospital deaths increased considerably.1 These changes varied by expected payer.2 It is important to determine whether overall hospital readmissions would also change given the impact of the COVID-19 pandemic on hospital care. This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents statistics on 30-day all-cause hospital readmissions among patients aged 1 year and older in the United States. Trends in readmissions by expected payer are provided from 2016 through 2020 using the HCUP Nationwide Readmissions Database (NRD). The brief presents changes in readmission rates from the pre-pandemic period of 2016-2019 to 2020 by select patient characteristics based on the index admission (i.e., the initial inpatient stay), including expected primary payer, patient location, and race and ethnicity. The brief also provides readmission rates and a comparison of costs for the index admission and the readmission for 2020 based on the principal diagnosis and grouped according to the Clinical Classifications Software Refined (CCSR) body system. Because of the large sample size of the NRD data, small differences can be statistically significant. Thus, only differences greater than or equal to 10 percent are discussed in the text. |
|
Findings
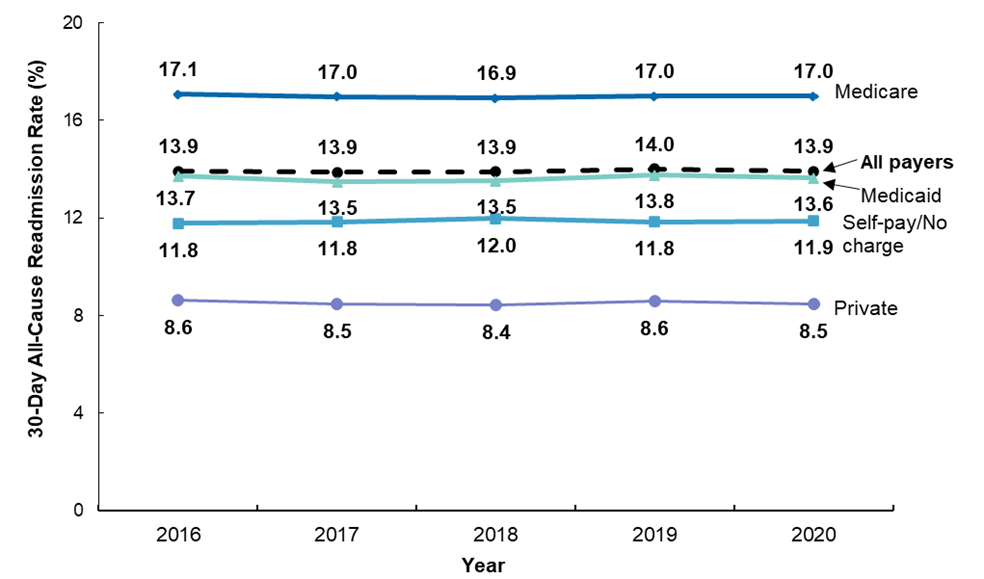
Rates of 30-day all-cause hospital readmissions by expected payer, 2016-2020 Figure 1 presents trends in the 30-day all-cause readmission rate by the expected primary payer from 2016 to 2020. The expected payer is determined by the index admission, not the readmission. Figure 1. Rates of 30-day all-cause readmissions by expected primary payer, 2016-2020
Table 1 presents the readmission rate and the number of readmissions by the expected primary payer and patient age group in 2016-2019 and 2020. Table 1. Rate and number of 30-day all-cause readmissions by expected payer and patient age group, 2016-2019 and 2020
a The expected payer is determined by the index admission, not the readmission. See the Definition section for a description of what is meant by the term expected payer.
Rates of 30-day all-cause readmissions by patient location and race/ethnicity, 2016-2020 Table 2 presents the 30-day all-cause readmission rate and the number of readmissions by the location of the patient's residence and by patient race and ethnicity in 2016-2019 and 2020. Table 2. Rate and number of 30-day all-cause readmissions by patient location and race/ethnicity, 2016-2019 and 2020
a The readmission rate is calculated using discharges from January through November to allow for a 30-day followup period.
Rates of 30-day all-cause readmissions by principal diagnosis, 2020 Tables 3 presents the 30-day all-cause readmission rate and the number of readmissions by the principal diagnosis at index admission for 2020. Principal diagnoses are ranked by the rate of readmission and grouped using the CCSR for the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) body system categories. Table 3. Rate of readmission for all causes within 30 days by principal diagnosis category at index admission, 2020
a Principal diagnosis at index admission is grouped by body system according to the (CSR, which categorizes the ICD-10-CM into a manageable number of clinically meaningful categories.
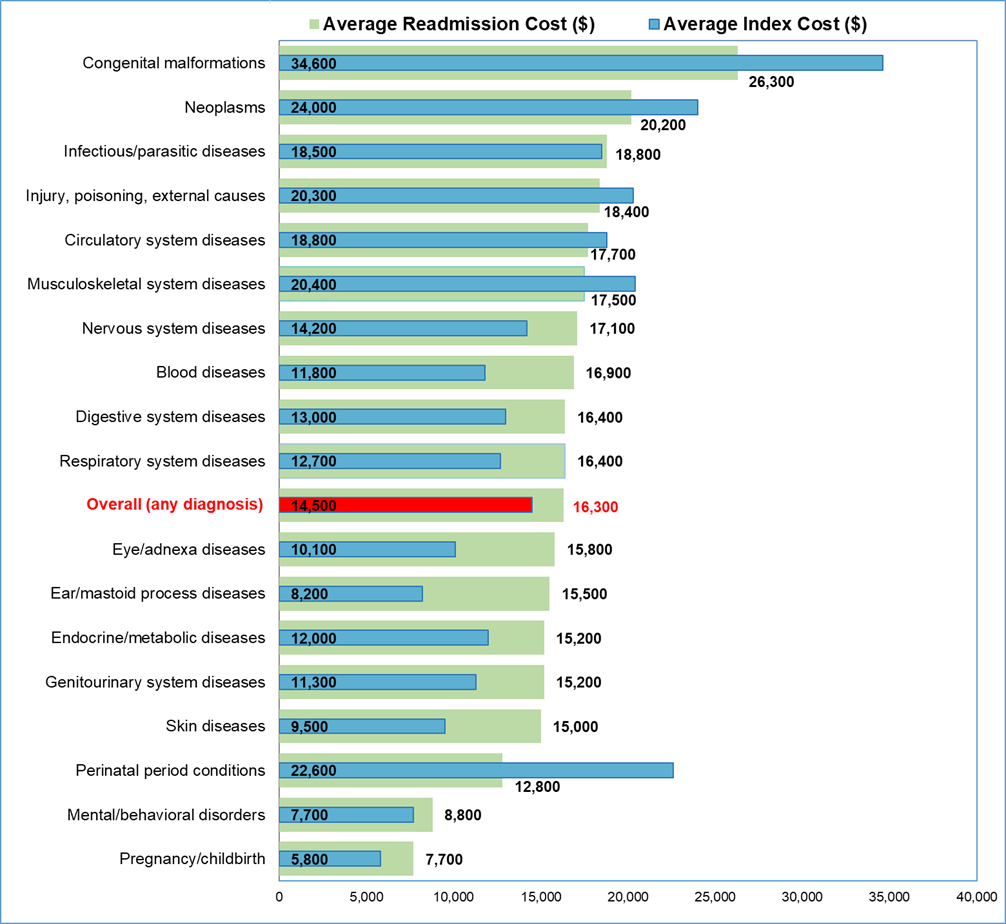
Average costs for the index admission and the readmission, 2020 Figure 2 presents the average cost of index admissions and the average cost of readmissions by principal diagnosis in 2020. Principal diagnoses are ranked based on the average cost of the readmission and grouped using the CCSR for the ICD-10-CM body system categories. Figure 2. Average cost of index admissions and 30-day all-cause readmissions by principal diagnosis category at index admission, ranked by average readmission cost, 2020
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References
|
|
About Statistical Briefs
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. |
|
Data Source
The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) 2016-2020 Nationwide Readmissions Database (NRD).
Types of hospitals included in the HCUP Nationwide Readmissions Database |
|
Definitions
Readmissions
Unit of analysis
Costs and charges
Percentage change
Expected payer
For this Statistical Brief, a hierarchy was used to assign the payer category based on the primary and secondary expected payer to give precedence to public payers (Medicare and then Medicaid) over commercial insurance.
Categorization of readmission counts by expected payer was based on the index stay. The concordance between the expected payer coded at the index stay and the expected payer coded at readmission varies by payer: 98 percent for Medicare, 95 percent for Medicaid, 93 percent for private, and 80 percent for self-pay/no charge (percentages based on the 2013 NRD).
Location of patients' residence
Reporting of race and ethnicity
Diagnoses
ICD-10-CM
Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses
Maternal/nonmaternal discharges |
The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels.
HCUP would not be possible without the contributions of the following data collection Partners from across the United States:
|
Alaska Department of Health Alaska Hospital and Healthcare Association Arizona Department of Health Services Arkansas Department of Health California Department of Health Care Access and Information Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Laulima Data Alliance Hawaii University of Hawai'i at Hilo Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute |
Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Health Authority Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources Wisconsin Department of Health Services Wyoming Hospital Association |
The HCUP Nationwide Readmissions Database (NRD) is a calendar-year, discharge-level database constructed from the HCUP State Inpatient Databases (SID) with verified patient linkage numbers that can be used to track a person across hospitals within a State. The 2010-2020 NRD are available for purchase through the HCUP Central Distributor. The NRD is designed to support various types of analyses of national readmission rates. The database includes discharges for patients with and without repeat hospital visits in a year and those who have died in the hospital. Repeat stays may or may not be related. The criteria to determine the relationship between hospital admissions are left to the analyst using the NRD. The NRD was constructed as a sample of convenience consisting of 100 percent of the eligible discharges. Discharge weights for national estimates are developed using the target universe of community hospitals (excluding rehabilitation and long-term acute care hospitals) in the United States. Over time, the sampling frame for the NRD will change; thus, the number of States contributing to the NRD will vary from year to year. The NRD is intended for national estimates only; no regional, State-, or hospital-specific estimates can be produced. The unweighted sample size for the 2020 NRD is 16,692,694 (weighted, this represents 32,336,475 inpatient stays). The unweighted sample size for the 2016 NRD is 17,197,683 (weighted, this represents 35,660,906 inpatient stays).
For other information on readmissions and revisits, refer to the HCUP Statistical Briefs topic area located at https://www.hcup-us.ahrq.gov/reports/statbriefs/sb_readmission.jsp.
For additional HCUP statistics, visit:
For more information about HCUP, visit www.hcup-us.ahrq.gov/.
For a detailed description of HCUP and more information on the design of the Nationwide Readmissions Database (NRD), please refer to the following database documentation:
Agency for Healthcare Research and Quality. Overview of the Nationwide Readmissions Database (NRD). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated October 2021. www.hcup-us.ahrq.gov/nrdoverview.jsp.
Jiang HJ, Hensche MK. Characteristics of 30-Day All-Cause Hospital Readmissions, 2016-2020. HCUP Statistical Brief #304. Rockville, MD: Agency for Healthcare Research and Quality; September 2023 www.hcup-us.ahrq.gov/reports/statbriefs/sb304-readmissions-2016-2020.pdf.
The authors would like to acknowledge the contributions of Minya Sheng, formerly of IBM Watson Health.
***
AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please email us at hcup@ahrq.gov or send a letter to the address below:
Joel W. Cohen, Ph.D., Director
Center for Financing, Access and Cost Trends
Agency for Healthcare Research and Quality
5600 Fishers Lane
Rockville, MD 20857
This Statistical Brief was posted online on September 22, 2023.
a Agency for Healthcare Research and Quality. Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). Updated November 3, 2021. www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed March 9, 2022.
b Agency for Healthcare Research and Quality. Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses. Healthcare Cost and Utilization Project (HCUP). Updated December 9, 2022. www.hcup-us.ahrq.gov/toolssoftware/ccsr/dxccsr.jsp